1. Introduction
he article describes the biomechanical aetiology of the so-called idiopathic scoliosis (1995 -2007), known as an adolescent idiopathic scoliosis (AIS). The first lecture dealing with the issue was delivered in Hungary in 1995. The first publication was made in Germany in 1996 (Orthopädische Praxis).
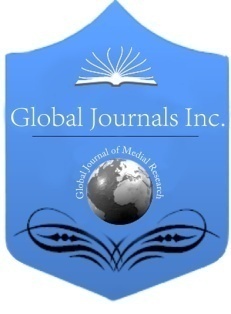
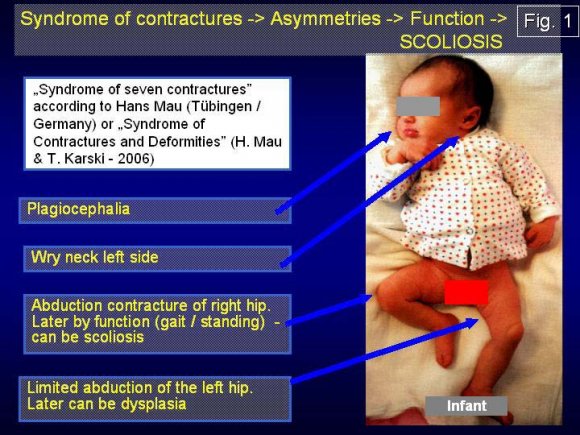
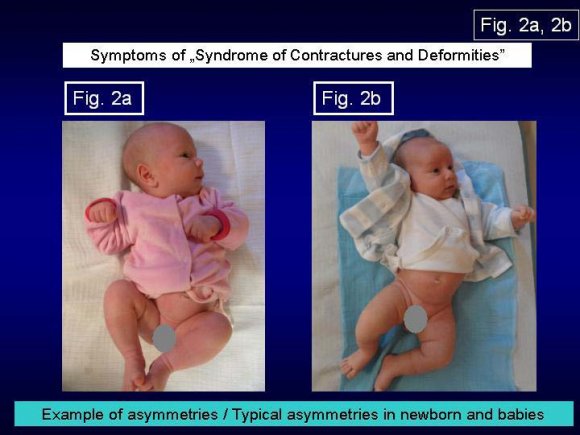
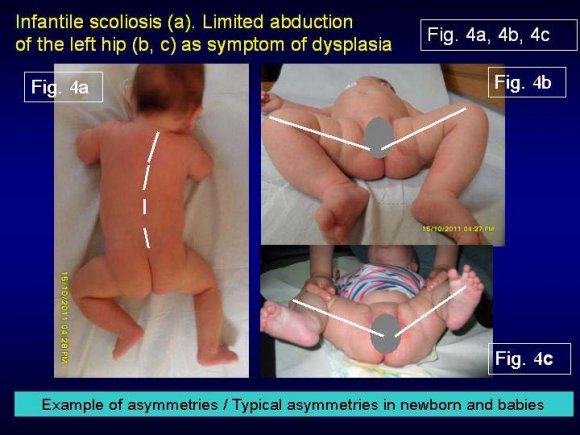
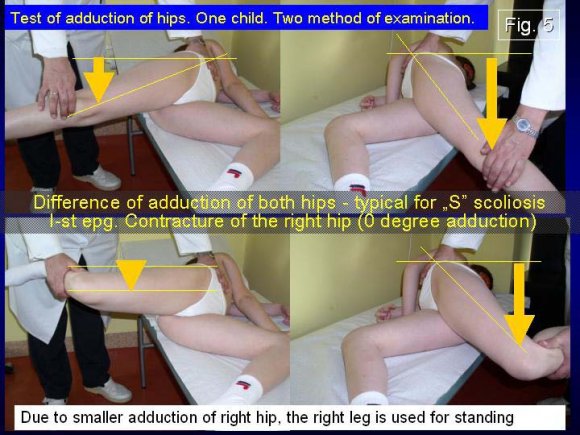
Biomechanical development of scoliosis. The scoliosis appears as the secondary deformity originating in the asymmetry of hips' position and movement described by Prof. Hans Mau in articles about Syndrome of Contractures (Fig. 1, 2a, 2b, 3, 4a, 4b, 4c). Nextwhile walking and while standing 'at ease' on the right leg (T. Karski). The research proves that the right leg is the preferred one over the years for standing. This phenomenon is because of better stability of right leg in region of right hip during standing and this is because of smaller adduction in straight position of joint. Every type of scoliosis starts to develop at the time when the child starts to stand and walk. Depending of types of scoliosis is a special characterise of patho-morphology of deformity of spine and their various properties. To explain in details the biomechanical aetiology we must remember about the three asymmetries causing the development of scoliosis: 1. The asymmetry of the movement in the hipsadductions test (Fig. 5) -is the primary cause for development of scoliosis. 2. The asymmetry of the movement and in loading in pelvis and spine -left versus right side in gait. Gaitinfluences factor in I epg scoliosis and in III epg scoliosis. 3. The asymmetry of the time while standing 'at ease' on the left versus the right leg -more time on the right leg. Standing on the right leg -influences factor in II/A epg scoliosis and in II/B epg scoliosis.
The asymmetry of movement of the hips is as mentioned above, is connected with "Seven Contractures Syndrome" described by Professor Hans Mau from Tübingen in Germany in 1960s (in German Siebenersyndrom) and then further explained (T. Karski) as a "Syndrome of Contractures and Deformities" (literature 1 -15).
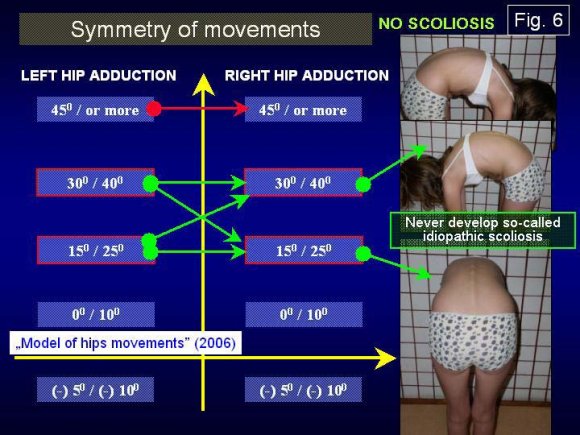
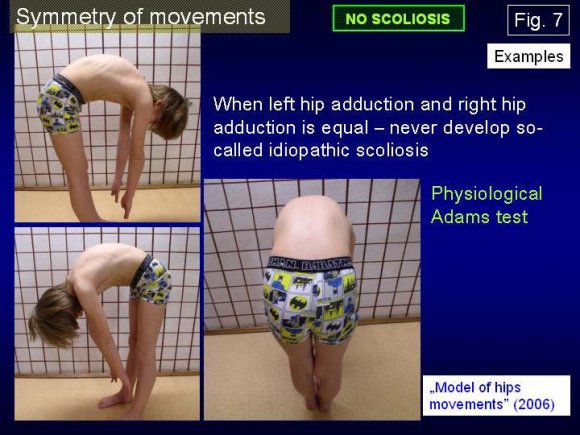
The consequential development of the spinal deformity is as follows: 1. Every type of scoliosis depends on the Model of Hips' Movement [MHM] (T. Karski 2006). 2. When the movement of hips is symmetrical -the is no pathological influence on spine during walking/gait and the is also symmetry of time standing on left / right leg. In such situation develop never so-called idiopathic scoliosis (Fig. 6, 7). 3. The asymmetry of the movement of hips in all cases of the so-called idiopathic scoliosis bases on the limited adduction, limited internal rotation and limited extension in the right hip. This phenomenon explain "the lest sided Syndrome of Contractures". 4. In gait, there is a limited movement of the right hip which is transmitted to pelvis and spine as a compensatory process and "enlarges" the movement in the spinal region. Consequently, there occurs a permanent distortion of the inter-vertebral joints, a rotation deformity and later stiffness of the spine. The asymmetry of the movement of hips in gait also causes a load asymmetry "with passing time" on both sides -left and right -and further, a gradual development of scoliosis. 5. The permanent standing 'at ease' on the right leg (the right hip is more stable [!]) starts and widens the curves -first, lumbar left convex and in II/B epg (see farther/next text) thoracic right convex curves. 6. The scoliosis "S" in I epg is connected with standing 'at ease' on the right leg and with gait. 7. The scoliosis "I" in III epg is connected only with gait. This type of scoliosis manifests itself as stiffness of spine. This deformity produces no curves or gibbous or a very slight one. 8. The following influences connected with gait and with standing on the right leg gives -three groups and four types of scoliosis (see above): "S" double scoliosis -I etiopathological group (epg); causal gait and standing on right leg, lumbar left convex curve in "C" -II/A scoliosis sometimes with secondary thoracic right convex curve in "S" -II/B epg scoliosis; causal standing on right leg. In this subgroup ("S" -II/B epg scoliosis) not only standing 'at ease' on the right leg is the cause of scoliosis but also the laxity of joints (typical for minimal brain dysfunction [MBD]) and harmful exercises in former therapy -before the stay in our Department. Asymmetry in the movements of hips (Tab. I). There are differences in the movement concerning the range of adduction, internal rotation and extension. (Tab. I) When movement of hips (see model of movements), especial adduction in strait position of joint (this position is important in function -in standing and in gait) -is equal its mean symmetric of both sides -there is no scoliosis.
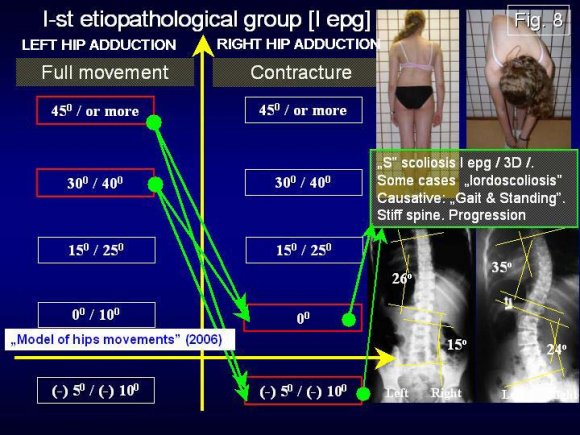
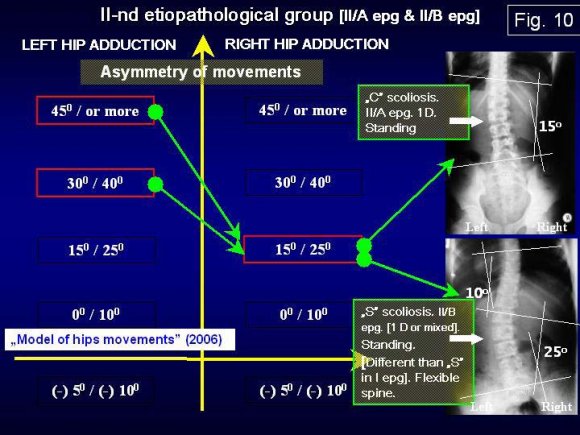
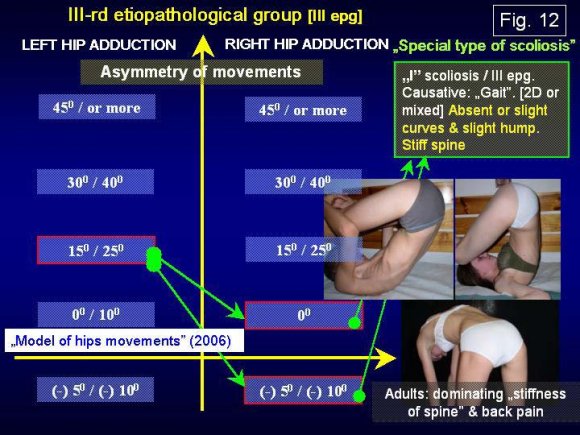
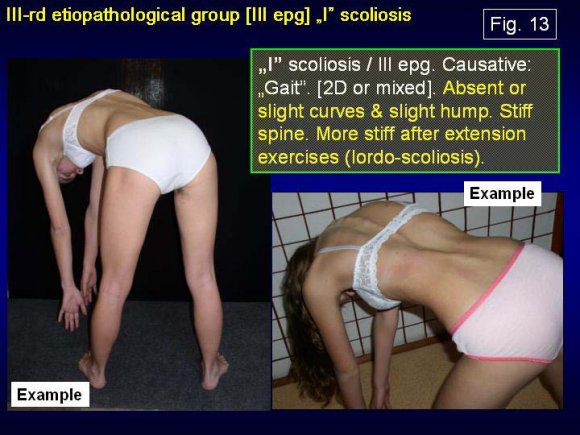
In new classification there are three groups and four types of scoliosis (Fig. 8, 9, 10, 11, 12, 13, 14). I / "S" double scoliosis with stiff spine (3D -I epg), connected with gait and standing 'at ease' on the right leg; IIA / IIB "C" and "S" scoliosis with flexible spine (II/A -1D & II/B -2D epg), connected only with standing 'at ease' on the right leg in "C" II/A epg and in "S" II/B epg additionally connected with laxity of joints and / or harmful previous exercises III / "I" scoliosis (III epg -2D) -stiff spine without curves and gibbous or with very slight ones. Connection with gait only. Every type of scoliosis starts to develop at the age of 2 or 3.
2. II. Comment to the New Classification
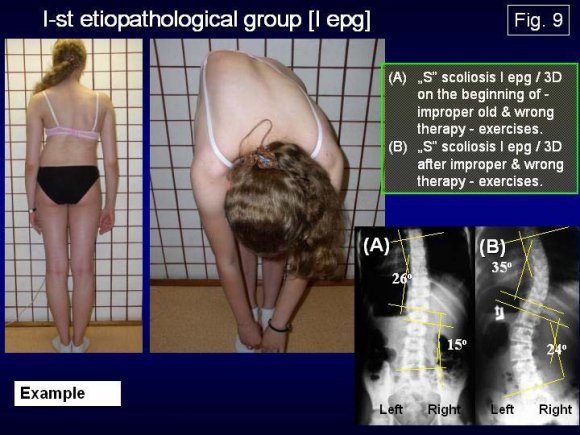
I-st etiopathological group of scoliosis is "S" deformity in I epg. (Tab. I). This scoliosis can be diagnosed very early, at the age of 3 to 5. The authors observed that children aged 1 year who can walk and stand independently, stand mostly 'at ease' on the right leg (observation in Out -Patient Clinic) and it should be an alarming sign for doctors and parents indicating / showing the beginning of the developing of scoliosis. In the I epg group, the first clinical sign is the rotation deformity which should warm against future spinal deformity. In some cases of I epg group there is "lordoscoliosis". The property of such scoliosis is: progression, especially after harmful exercises.
II-nd etiopathological group of scoliosis -"C" II/A epg deformity and "S" II/B epg deformity (2001). The scoliosis in II/A epg or II/B epg can be diagnosed at the age of 8 -10 -12 (Tab. I). The cause is the habit of permanent standing 'at ease' on the right leg for many years. Initially, it is the lateral physiological deviation, then fixed "C" left convex curve. In the development of the "S" II/B epg scoliosis there occurs additionally laxity of joints and / or harmful exercises (mentioned above). In some cases of II/B epg group we observe kypho (kifo) -scoliosis.
III-rd etiopathological group of scoliosis ( 2004)scoliosis with little or no curvature (Tab. I). The cause is connected only with gait. In gait due to a restricted movement in the right hip, and a small movement in the left hip, a compensatory rotation movement in the spine is created. This compensatory movement makes, as mentioned above, a permanent distortion in the intervertebral joints which result in stiffness and rigidity of the whole spine. The stiffness of the spine can be observed in youth. However, nobody considered this to be scoliosis. These patients when adult often suffer from back pain.
The necessity of causal prophylaxis. The new classification clarifies the need for therapeutic approach to each etiopathological group of scoliosis and provides the possibility to introduce causative prophylaxis which is the theme of the next two lectures. III.
3. Conclusions
1. Last 39 years of Lublin observations confirmed the biomechanical aetiology of scoliosis. 2. There are three types and four groups of scoliosis connected with causative influence "standing on the right leg at ease" (treated as "standing") and with "walking" (gait). 3. There are following types of scoliosis: "S" scoliosis I epg, 3D

| Model of | Causative | Type of "S" | Type of "C" | Type of "S" | Type of "I" |
| hips | influence | scoliosis -I | scoliosis - | scoliosis - | scoliosis -III |
| movements | epg | II/A epg | II/B epg | epg | |
| Range of add. | Gait and | Scoliosis "S" | |||
| right hip -10 / | standing on | I epg | |||
| -5 / 0 degree | the right leg | Two curves. | |||
| Range of add. | 'at ease' | Rigid spine. | |||
| left hip 30 / | (free) | Gibbous in | |||
| 40 / 50 degree | thorax right | ||||
| side. 3D. | |||||
| Progression. | |||||
| Range of add. | Standing on | Scoliosis "C" | Scoliosis "S" | ||
| right hip 20 / | the right leg | II / A epg. | II / B epg. | ||
| 30 degree | 'at ease' | Lumbar or | Lumbar left | ||
| Range of add. | (free) | Sacro - | convex. | ||
| left hip 40 / | Lumbar or | Thoracic | |||
| 50 degree | Lumbar - | secondary | |||
| Thoracic left | right convex | ||||
| convex curve. | curve. | ||||
| Flexible | Flexible | ||||
| spine. 2D. No | spine. 2D or | ||||
| progression or | 3D. No | ||||
| small. | progression or | ||||
| amall. | |||||
| Range of add. | Gait | Scoliosis "I" | |||
| right hip -10 / | III epg | ||||
| -5 / 0 degree | No curves or | ||||
| Range of add. | slight. | ||||
| left hip 0 / 10 | Rigid spine. | ||||
| / 20 degree | 2D or 3D. | ||||
| Stable | |||||
| deformity. | |||||
| Not included | |||||
| till now to | |||||
| "scoliosis". |