1. Management of Malignant Renal Cyst -Nephrectomy Case Presentation
Dr. Nexhat Shabani ? , Prof. Dr. Mustafa Xhani ? , Dr. Albesa Shabani ? & Dr. Rrezart Xhani ? I. Introduction enal cysts, in general, may be classified as "simple" or "complex". "Simple" cysts are best defined using sonographic criteria. The difficulty arises when cysts do not meet the rigid characteristics of the "simple" definition. Therefore, clinicians need to rely on a rapid, safe and accurate system to identify benign versus malignant masses and ultimately have the guidance on nonsurgical or surgical treatment options. Malignant renal cyst is a very rare disease. In literature are prescribed as 0.5-1% of all renal cysts (1,2). Their clinical symptoms are not specific and are mainly similar to the symptomatology of tumors and simple renal cysts (3,8). Pre operative diagnostics procedure as intravenous urography -IVU, ultrasonic sonography, computed tomography-CT, magnetic resonance imaging -MRI, diagnostic punction of cysts and renal arteriography can rare determine the diagnosis (4,5). The diagnosis based on Bosniak classification: Bosniak 1, Bosniak 2, Bosniak 2F, Bosniak 3 and Bosniak 4. Therefore the diagnosis is mostly determined by surgical intervention (6,7). In this study, the authors have presented their case of hemorrhagic malignant renal cyst, which is treated by surgical intervention -nephrectomy.
2. II. Objective
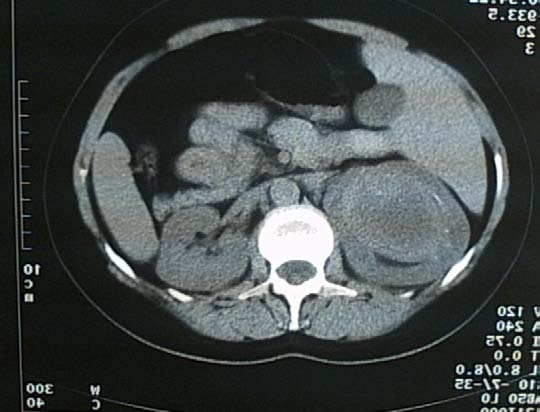
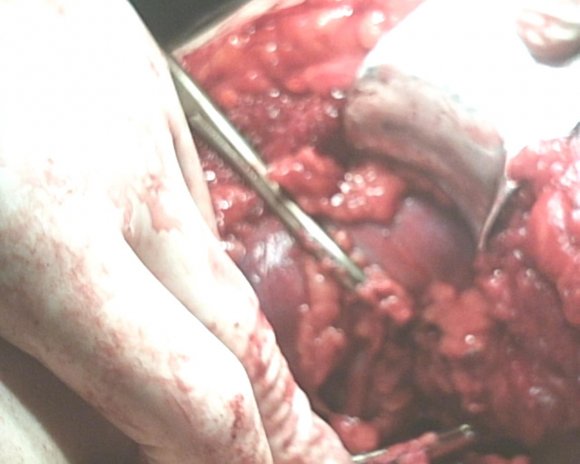
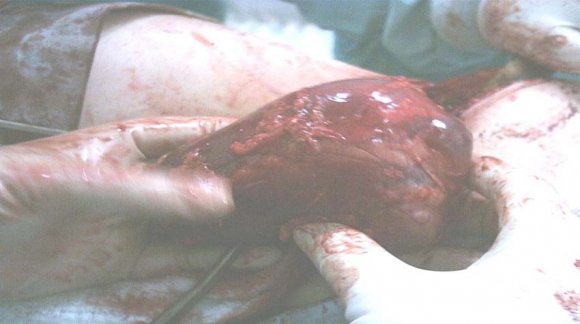
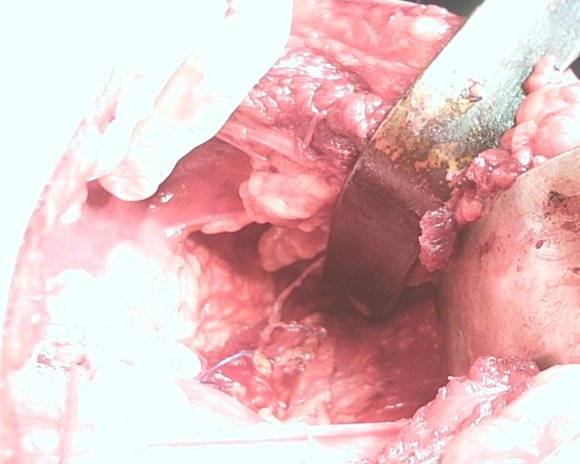
A case of malign hemorrhagic renal cyst in a 32 -year -old woman is reported. The patient was admitted to our hospital for further evaluation of right upper abdominal mass. CT scan and ultrasonic sonography showed a right giant renal cystic mass. The characteristic findings were thick and irregular wall and heterogeneous contents of the cystic mass. The presence of a malignant tumor in the cyst wall was suspected and nephrectomy was performed. The specimen measured 10 x 6 x 4 cm. The cyst contained bloody fluid and a hemorrhagic degenerating mass. Pathohistological examination showed evidence of malignant hemorrhagic renal cyst.
3. III. Patient and Methods
We are going to present the case of a female patient referred to our clinic with the initial ultrasound Author ? ? ? ?: Urology Department, Regional Hospital -Gjilan, UHC "Mother Theresa" Tirana, Albania, SLK Kliniken, Internal Medicine, Heilbronn, Germany. e-mail: [email protected] diagnosis of right giant renal cyst about 10 cm. Physical examination revealed no abnormalities. Given the result of the ultrasound (thick walls and small irregularities) and the possibility of a complicated cyst, we decided to investigate the matter further, and programmed the patient for an enhanced abdominal computer tomography with intravenous contrast.
The enhanced CT images revealed a right kidney cystic mass, with a 10 cm diameter, thick irregular walls with contrast enhancement, hyperdens content, and no pathological lymph nodes or distant metastases. The diagnosis was a Bosniak IV.
4. IV. Bosniak Classification of Cystic
Renal Masses
5. VI. Discussion
Diagnosis is mainly based on histopathological features such as a well-developed capsule, fibrous stromata, multiple epithelial lining septa. According to Bosniak the renal cysts can be classified into 5 types. A simple renal cyst grows up of renal parenchyma. The cyst is filled with fluid and can cause local tissue destruction as it enlarged. Many cysts cause no symptoms and are discovered accidentally during other assessment or autopsy. Although the exact cause is unknown, cysts are considered structural defect that occurs prenatally. Diagnosis of a simple renal cyst involves intravenous urography, echosonogarphy, diagnostic puncture, CT, MRI. Echosonogarphy is the most commonly applied method because it reveals some features of cysts of suggesting malignancy: irregular walls, internal echoes inside the walls and the cysts, lack of characteristic potentiation of ultrasound beam (F).This indicate diagnostic punction and analysis cyst contents. If the aspirate is bloody there is (Tomas¹ 2010) a 28 -5o % chance of malignancy.
6. VII. Conclusion
The characteristic findings were thick and irregular wall and heterogeneous contents of the cystic mass. The cyst contained bloody fluid and a hemorrhagic degenerating mass. Pathohistological examination showed evidence of malignant hemorrhagic renal cyst. Which is treated by surgical intervention and usually nephroctomy.