1. I. Introduction
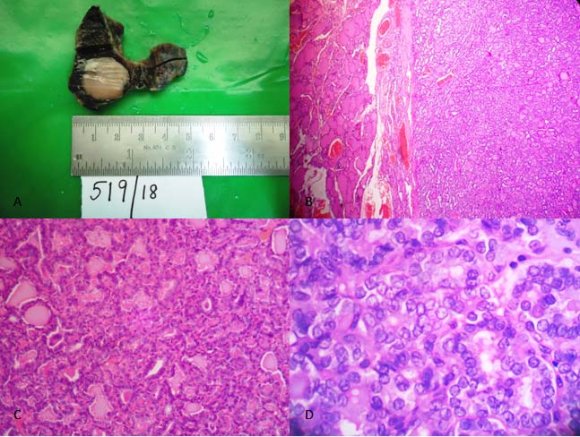
he fourth edition 2017 of the WHO book on the classification of the tumors of endocrine organs includes new entity 'Non Invasive follicular neoplasm with papillary like nuclear features' (NIFTP). [1] This was done additionally to characterize the clinical behavior of this lesion, thus further helping to predict prognosis and manage the patients appropriately. Hence overall helping to prevent overtreatment and decrease the cancer diagnosis burden. [2] The WHO has coded unspecified, borderline or uncertain behavior for NIFTP. Hence it is a neoplasm, but not cancer. NIFTP presents mostly similar to other thyroid neoplasms by detection of a nodule on routine examination or incidentally on imaging. Histopathology shows solid, well-circumscribed or encapsulated nodule. Diagnosis is made by strict inclusion and exclusion criteria following submission of the entire capsule for histology and carefully examining the nuclear and architectural features, (Table -1). [3] II. Case Report Forty years old female presented with the complaint of neck swelling from the past few months. Her ultrasonography neck was suggestive of multinodular goiter. Her thyroid function tests were normal. Fine needle aspiration cytology was suspicious of papillary carcinoma. She underwent total thyroidectomy at Mohandai Oswal cancer hospital. The specimen was recieved for histopathological examination at Oncquest laboratories, situated in Mohandai Oswal cancer hospital. Specimen measured 4.3x4x2cm. The left lobe measured 4x2x2cm. On cut section, it showed a well-circumscribed nodule measuring 1.7x1.7x1.3cm, which was paler than the surrounding thyroid parenchyma. Grossly areas of hemorrhage or necrosis were absent. The right lobe and isthmus showed unremarkable morphology. Sections of the nodule with capsule were embedded. Sections from the left lobe showed encapsulated neoplasm containing medium-sized follicles lined by cuboidal cells displaying nuclear clearing, overlapping and grooving in few cells. An occasional intranuclear inclusion was noted. However, psammoma bodies, tumor necrosis, and mitosis were absent. Papillary architecture (<1%) was noted. Re-grossing was done. Entire nodule and capsule were submitted. Sections showed no capsular or vascular invasion. Hence the final diagnosis of Non Invasive follicular thyroid neoplasm with papillary like nuclear features (NIFTP) was given.
2. III. Discussion
WHO 2017 fourth edition stated NIFTP as a neoplasm of unspecified, borderline or uncertain behavior. Also, the word cancer was therefore omitted. [1] This new terminology reflects key histopathological features of this lesion that is of invasion, follicular growth pattern and nuclear features of papillary thyroid carcinoma. These tumors do not show molecular alterations associated with classical papillary thyroid carcinoma, such as BRAF V600E mutations. However, these demonstrate RAS and other mutations associated with follicular pattern thyroid tumors. [4] The treatment for NIFTP is simple lobectomy, near total or total thyroidectomy. No further surgery is needed. No postoperative radioactive treatment is given. The major advantage of NIFTP for cytology is the reduction of SM category (Suspicious for malignancy Bethesda category V) diagnosis. In follicular patterned tumors it is very much dependent on good quality smears and the cytopathologist expertise. The main disadvantage is the false negative diagnosis in the SFN/FN (Follicular Neoplasm or Suspicious for a Follicular Neoplasm Bethesda category IV) leading to the need of a second surgery for total thyroidectomy in cases of the infiltrative follicular variant of papillary thyroid carcinoma (I-FVPTC). [5]
3. Global
4. IV. Conclusion
With this approach in mind, the ability to differentiate NIFTP from classical papillary thyroid carcinoma will facilitate the conservative surgical management of the patients without radiotherapy or prophylactic central lymph node staging and with more studies adding to the evidence of good prognosis of these tumors. [3,6] Therefore this nomenclature change will reduce mental burden, overtreatment, financial burden, and other cancer diagnosis related consequences.
5. Legends:
Table 1: Diagnostic Criteria for NIFTP [3].
| 1. Encapsulation or clear demarcation * a . |
| 2. Follicular growth pattern * b with : |
| ? <1% Papillae. |
| ? No psammoma bodies. |
| ? <30% Solid/trabecular/insular growth pattern. |
| 3. Nuclear score 2-3. |
| 4. No vascular or capsular invasion * c . |
| 5. No tumor necrosis. |
| 6. No high mitotic activity * d . |
| *a -Thick, thin, or partial capsule or well |
| circumscribed with a clear demarcation from |
| adjacent thyroid tissue. |
| *b -Including microfollicular, normofollicular, or |
| macrofollicular architecture with abundant |
| colloid. |
| *c -Requires adequate microscopic examination of |
| the tumor capsule interface. |
| *d -High mitotic activity defined as at least three |
| mitoses per 10 high-power fields (X400). |