1. Introduction
vascular necrosis(AVN) is the cellular death of the bone due to various factors causing vascular compromise. This vascular compromise leads to ischemia and cell death which will result in relentless progression of the disease. Femoral head is the most commonly affected site as it is the weight bearing part of the bone and due to its precarious bloodsupply.AVN of the femur is one of the common causes of hip pain presenting in young age. Some of the common risk factors associated with AVN include trauma, corticosteroid use, chronic alcoholism, pancreatitis, sickle cell disease, gout, radiation, SLE (1,2).
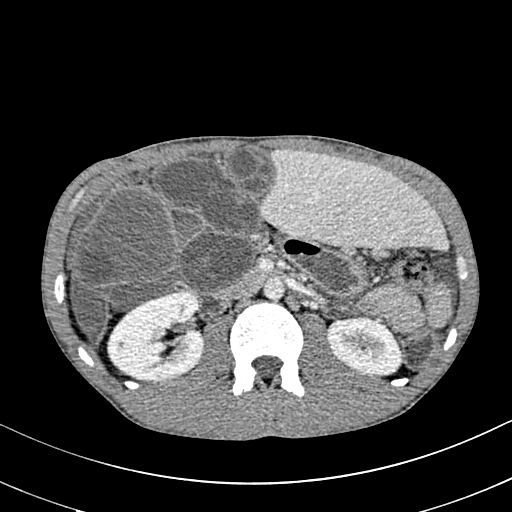
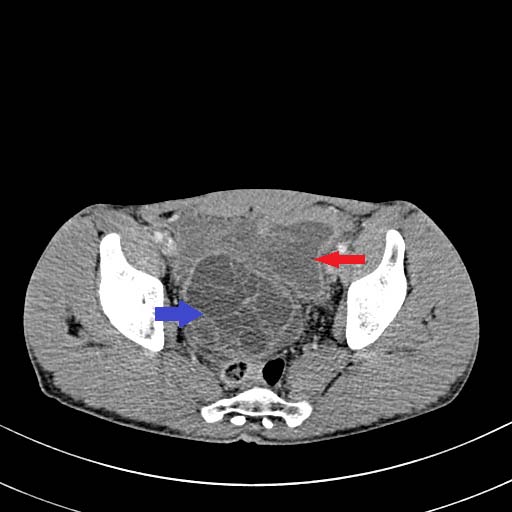
Radiologic staging of the disease is of crucial importance in the identification and risk stratification in pre-collapse stages, prognosis, treatment planning, and post-operative follow-up. Radiograph of the pelvis with both hips is the first imaging usually done in a suspected case of AVN, but unfortunately, plain radiographs are of no much use in early stages of AVN (3). MRI is the most sensitive imaging modality in diagnosing AVN. It is the investigation of choice for the definitive staging of AVN, because images clearly portray the size of the lesion, and overall estimates of the stage of disease can be made. CT is usually done to assess the extent of disease and to look for subchondral fractures or collapse.( 4) SPECT scanning has a role in determining the radioactivity of the organ and it is beneficial in early cases to spot the avascular focus that can be un noticed with routine plain MRI sequences. Bone scanning is advised in cases where MRI is contraindicated or equivocal, and it is useful in quantifying the physiologic data i.e., uptake in static and perfusion states. Bone biopsy is accurate, and can diagnose early, however, usually avoided as it is invasive (7).
2. II.
3. Materials and Methods
This single-center retrospective observational study was conducted in the department of radiodiagnosis in a tertiary care institute situated in an urban area. 70 patients of all age groups with clinical suspicion of AVN were evaluated over a period of one and a half years between January 2020 to June 2021. Of these, 6 patients with features of osteoarthritis were excluded. Demographic details like age, gender and clinical symptoms were collected. Clinical details with particular emphasis on the risk factors for AVN and relevant lab parameters were collected from records and reviewed for all patients. Scans were performed on 3 Tesla MRI scanner, Siemen's SkyraTM. Ficat and Arlet classification was used to stage the avascular necrosis of the femoral head.
4. III.
5. Results
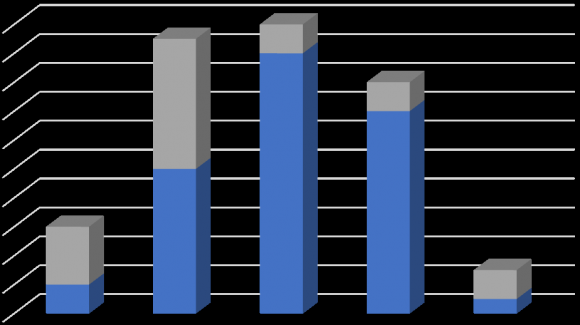
In this study of 64 patients with osteonecrosis of femoral head, 41(69%) were males and 18 (31%)were females with male to female ratio of 2.2:1. Prevalence of AVN was found to be highest in the economically productive age group of 21 to 40 years (62.7%) i.e 37 cases, 5(8.4%) cases belongs to age group of 11-20 years,14 (23.7%) cases belongs to the age group of 41-50 years and 3(5%) cases belongs to the age group of 51-60 years. The mean age of presentation was found to be 33.98+/-10.03. There is no statistical significance between the mean ages of presentation in males and females (M=35.05,F=30.67).
Graph 2: Age wise distribution of cases.
In the present study, The presentation was bilateral in 48(81.3%) and unilateral in 11(18.6%) cases. The analysis of risk factors in our study demonstrated that chronic alcoholism (35.5%) was the most common risk factor associated with AVN of femoral head followed by chronic steroid use (25.4%).
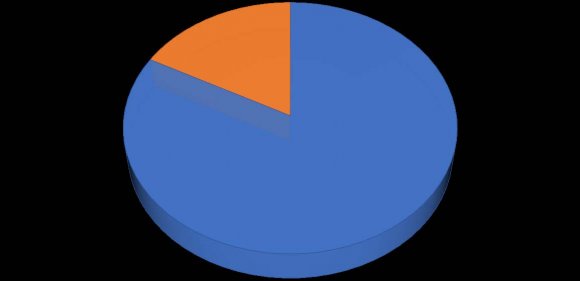
other risk factors include Idiopathic(16.9%), sickle cell disease( 6.7%), systemic lupus erythematosus(6.7%), trauma (5.08%), diabetes(1.69%). In this study, anterosuperior quadrant was involved in 72 (62%) of femoral heads followed by superior quadrant in 32 (27%), entire head was involved in 11(9%) heads, anteromedial and infero medial quadrants were involved in1 (1%) femoral heads each. Analysis of MRI findings revealed that double line sign was most common finding seen in 85%femoral heads followed by loss of contour in 62%of heads, joint effusion was seen in 60% heads,bonemarrow edema in 50% and joint space reduction was noted in 18% of femoral heads.
6. ENTIRE HEAD 9% [CATEGORY NAME] [PERCENTAGE] [CATEGORY NAME] [PERCENTAGE]
7. ANTEROSUPERIOR SUPERIOR ENTIRE HEAD ANTEROMEDIAL INFEROMEDIAL
Table 1: Analysis of MRI findings in AVN Association of Joint effusion with staging showed that joint effusion was more common in stage 3and 4 that is 77% and 47.6% respectively followed by stage 2 in 46.5 %of femoral heads. A total of 70 out of 117 femoral heads showed joint effusion ie; 59.8%.
8. Table 2: Association of joint effusion with staging
Association of marrow edema with staging showed that marrow edema was more common in stage 4 seen in 57.1% followed by stage 2 and 3 ie; 49 and 48 percent respectively.
9. Discussion
In this retrospective observational study of 64 patients, 45(70%) were males and 19(30%) were females with male to female ratio of 2.2:1. It shows higher prevalence of AVN in male than female population. This observation was similar to the study conducted by Jyothi choudary et al (1) in which 69% of the affected cases were males and 31% were females.
In our study AVN was found between age groups of 13 to 6o years with most of the patients 39(61%) belong to the age group of 21-40 years as the risk factors for AVN such as alcohol and steroids use most frequently occur in this age group. 16(25%) patients belong to the age group of 41 -50, 3(4.6%) patients belong to the age group of 51-60 years and 6(9.3%)patients belongs to the age group of 11 -20.
The mean age of presentation was 34.2 years which is similar to the study conducted by Harsha vardhan et al (7) where the mean age was 34.7 years. There is statistically significant difference in the mean age of males and females with females being affected at a relatively younger age than males (P<0.05).
Bilateral disease 53 (83%) was more common than unilateral involvement 11(17%) in this study.
According to Ficat & Arlet classification of AVN, out of 117 femoral heads involved, we observed stage III was the commonest stage seen in 52 (44.4%) femoral heads followed by stage II in 43(36.7%) femoral heads. This was similar to study conducted by Jyothi choudary et al (1), in which stage III AVN was found in 39.4% femoral heads followed by stage II in 30.4% heads.
In this study, we found that alcohol was the most common associated risk factor for the avascular necrosis of femoral head seen in 23 patients (36%).
This finding is consistent with the study conducted by Mohammad Zeeshan Saleem et al(2) and Jacobs et al (6), in which alcohol was the most common associated risk factor in 56% and 39% respectively. The mean duration of intake of alcohol was 82 months in our study. In a study conducted by Harshavardhan et al (7), the mean duration of alcohol intake was 88months.
The exact mechanism of alcohol causing AVN is not known. However several studies have concluded that fat embolism linked to hyperlipidaemia which in turn leads to the blockage of blood supply to femoral head and eventually bone death.
The next common associated risk factor in our study is corticosteroid use in 17 patients (27%). Harsha Vardhan et al (7) in their study concluded that steroid was the most common risk factor associated with AVN.
The most common indication for steroid intake in out institute was SLE. Other indications include rheumatoid arthritis, glomerular nephritis, nephrotic syndrome, renal transplant, auto immune haemolytic anaemias, paraquet poisoning.
Though the pathogenesis of steroid induced AVN is not fully understood, the postulated mechanisms include fat hypertrophy, fat emboli and intravascular coagulation that leads to the impaired blood supply to bones.
Other risk factors in our study were sickle cell disease in 4(6%) patients, SLE in 4(6%) patients, trauma in 3(5%) patients, diabetes in 1(2%) patients and no identifiable cause was observed in 12 (19%) patients.
In this study 2 patients of sickle cell disease showed multiple bone infarcts involving iliac bones in addition to the AVN of femoral head. The most common quadrant involved in our study is anterosuperior quadrant seen in 62% of the heads followed by superior quadrant in 27 % cases.
Gabriel et al (5), in their study showed that involvement of anterosuperior quadrant is specific for AVN. Nishii et al (3), in their study showed that location and size of the lesion are the prognostic indicators of collapse and large necrotic lesions have likelihood to involve anterosuperior quadrant.
In this study most common MRI finding of AVN is double line sign seen in 99 femoral heads (85%) which is considered pathognomic of AVN.
Other common findings are contour loss(62%), joint effusion (70%), bone marrow edema(50%), joint space reduction(18%).
In our study, joint effusion is seen in 70 out of 117 femoral heads(60%). The results of our study indicate that joint effusion is more prevalent in advanced stages of disease ie. stage III and stage IV. Out of 52 heads in stage III, 40 heads had joint effusion(76.9%) and out of 21 heads in stage IV, 10 heads had joint effusion(47.6%). 20 out of 43 heads of stage II heads had joint effusion(46.5%). Gou Chu Huang et al(8) and Mohammad Zeeshan Saleem et al (2), showed that stage III disease was most common to have joint effusion.
Bone marrow edema is seen in 50 out of 117 femoral heads(50.4%).
The results of our study showed that marrow edema is more prevalent in stage IV(51.1%) followed by stage II(48.8%) and stage III(48%).
In this study we have observed that 41 out of 59 osteonecrotic hips with marrow edema (81.3%) had associated joint effusion. The presence of joint effusion and bone marrow edema are prognostic factors for collapse. S Iida et al(4),In their study concluded that bone marrow edema was highly correlated with subsequent collapse.
V.
10. Conclusion
As osteonecrosis of femoral head is increasingly becoming the cause of Musculoskeletal disability especially in younger age group, its early diagnosis is crucial because early interventions are associated with better prognosis.
This study shows that MRI is the imaging modality of choice. It helps in early diagnosis and better outcome and can also visualize the bone marrow changes, location and extent of area involved which are helpful when ascertaining patient prognosis and formulating plan of care.