1. I. Introduction
riglyceride (TG, triacylglycerol, TAG or triacylglyceride) is an ester derived from glycerol and three fatty acids. Triglycerides are a blood lipid that helps enable the bidirectional transference of adipose fat and blood glucose from the liver. There are many triglycerides depending on the oil source. Some of these are highly unsaturated in the human body; high levels of triglycerides in the bloodstream have been linked to atherosclerosis and by extension, the risk of heart disease and stroke [1].
Hypertriglyceridemia is a prevalent risk factor for cardiovascular disease (CVD) and increasingly important in the setting of current obesity and insulin resistance epidemics. High triglyceride (TG) levels are markers for several types of atherogenic lipoproteins. Patients who have hypertriglyceridemia may be at significant risk for CVD even if low-density lipoprotein cholesterol levels are at goal, and therefore warrant treatment that optimizes diet, reduces overweight, and promotes regular exercise [2].
High-risk patients with hypertriglyceridemia, such as those with diabetes, CVD, or metabolic syndrome, may benefit from additional drug treatment aside from a statin to address other lipid abnormalities. In this discussion, we review the role of hypertriglyceridemia and its associated atherogenic lipoproteins in the pathogenesis of atherosclerosis, the relevance of a high TG level as a predictor of CVD, the cardiovascular outcomes from TG-lowering intervention trials, and the current guidelines for treating hypertriglyceridemia [3].
Men and women who have high triglyceride levels >150 mg/dl and a low level of HDL cholesterol <40 mg/dL are characterized by a significantly increased cardiovascular risk. The high triglyceride/low HDL cholesterol phenotype is a hallmark of the metabolic syndrome. The metabolic syndrome is closely associated with insulin resistance and is highly associated with the risk of CHD. It has a greater impact on the incidence of CHD in women than in men [3].
Adipose cells which make up adipose tissue are specialized cells which contain and can synthesize globules of fat. This fat either comes from the dietary fat we eat or is made by the body from surplus carbohydrate or protein in our diet. Adipose tissue is mainly located just under the skin, although adipose deposits are also found between the muscles, in the abdomen, and around the heart and other organs. The location of fat deposits is largely determined by genetic inheritance. Thus it is not possible to affect where we store fat. Nor is it possible to influence from which area the body burns fat for energy purposes [4]. Respective of the location from which they are obtained, the fat cells in humans are composed almost entirely of pure triglycerides with an average density of about 0.9 kilograms per liter. Most modern body composition laboratories today use the value of 1.1 kilograms per liter for the density of the "fat free mass", a theoretical tissue composed of 72% water (density = 0.993), 21% protein (density = 1.340) and 7% mineral (density = 3.000) by weight [5].
Fat cells are not only energy depots, but are busy endocrine organs. They secrete cytokines, which regulate responses to infection, immune reactions, inflammation and trauma. In regards to inflammation regulation, fat cells secrete pro-inflammatory (TNF, IL-6, and C-reacting protein "C-RP") and anti-inflammatory (adiponectin) cytokines. Unfortunately, with visceral fat obesity accumulation, adiponectin levels are reduced, thus leading to a higher cardio metabolic disorders (e.g., heart disease and diabetes [3]. Low intensity low frequency (LILFU) stands for low intensity, low frequency ultrasound. It is a new technique devised by the team of William Tyler from Arizona State University to manipulate neural circuits using ultrasounds. This could make in the future the need of intervention (surgical) neuromodulation unnecessary [8].
2. Fig. (4) : The relation between ultrasound frequency and penetration
Cavitation is the process in which a bubble in a fluid is forced to oscillate in size or shape due to some form of energy input, such as an acoustic field. Such cavitation is often employed in ultrasonic cleaning baths and can also be observed in pumps, propellers [8].
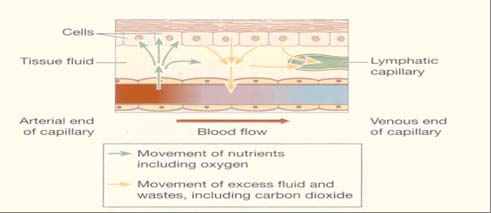
Lymph carries away large particles bacteria, Cell debris which can then be filtered out and destroyed by the lymph node Lymph capillaries in the interstitial spaces have same structure as blood capillaries but their walls are more permeable to inter stitial fluid constituents [9]. Moreover, nearly all lymph nodes are embedded in adipose tissue and most peripheral adipose depots contain one or more lymph nodes as well.44. However, whether there is a causal relationship between lipid content in the lymph and fat deposition is not known [10].
What seems to become clear, however, is that lymph stasis and ? or fluid leakage from lymphatic vessels may promote fat accumulation.45 In our experience, when intestinal lymphatic drainage was interrupted by heat cauterization of guinea pig mesenteric vessels, an obvious increase in mesenteric adipose tissue deposition occurred over a 28-day period.46. This observation is reminiscent of what occurs during lymphedema, where lymphatic drainage is disrupted or malfunctioning [11].
The fatty acids found within lymphocytes of lymph nodes upon stimulation come mainly from triacylglycerol's in the immediately adjacent perinodal adipose tissue, which contains more polyunsaturated fatty acids than fat further from lymph nodes [10].
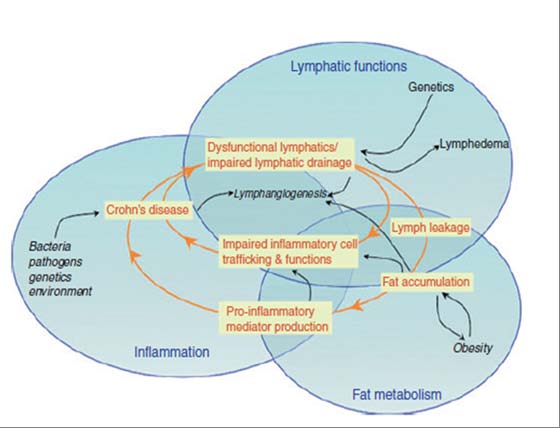
The relationships between the lymphatic system, adipose tissue, lipids profile and immune response ?inflammation are undeniable. Our current understanding of the cross-talk between these systems and illustrates how disturbance of these interactions may contribute to the pathogenesis of many disease [11]. 6) : Proposed working model for the interactions between lymphatic, fat and inflammation [11].
As the lymphatic system is the platform for the immune system and lymph nodes are the sites of adaptive immune responses modulated by the surrounding adipose tissue, increased knowledge of how the lymphatic system contributes to triglycerides transport, distribution and metabolism and to the pathogenesis of chronic inflammatory conditions may provide the basis for the development of new therapeutic strategies and increased quality of life [11].
3. II. Methods and Procedures a) Participants
The study was carried on 40 female patients with age ranges from 40 to 50 years were selected from Palestine hospital, They were obese atherosclerotic patients and were assigned into 2 groups according to their BMI based on the classification of the world health organization, Each patient in the two groups (class I and class II) was evaluated before and after 24 sessions treatment program by using the combination of ultrasound and lymphatic drainage machine. The assessment of blood serum triglycerides by UDICHEM-300 Chemistry Analyzer have been done before and after the end of 24 sessions and Re-assessment after 2 months from the last treatment session. ? Blood sample will be collected and investigated in the laboratory before and immediately after the treatment course and re-estimated two months late.
A three milliliter-sample of venous blood was drawn from the antecubital vein after 12-14 hours fast from all patients before the initiation of the training program and after the completion of the study (i.e. at the end of the 24 sessions) and re-assessed 2 months after the end of the program to be assayed for measurement of serum level of fasting Triglycerides.
4. a) General Characteristics
Class I: include twenty female patients with age ranges from 40 to 50 years old with the mean value of (46 ± 3.77) yrs, the weight ranged from 80 to 100 Kg with the mean value of (98.5 ± 6.67) kg, the height ranged from 150 to 160 cm with the mean value of (158 ± 5.06) cm. The BMI ranged from 35 to 39.9 kg/m2 with the mean value of (38. 3 ± 1.98) kg/m2 as shown in Table To determine the differences in the mean values of total body triglycerides among the groups, repeated measure analysis of variance (AVOVA F-Test) was performed as shown in Table (1) showed the f-test result.
5. Fig. (14) : Comparing the mean values of Total Body Triglycerides among the two groups
The results of the class I and class II groups revealed that, there is a significant improvement (reduction) in the Total Body Triglycerides for the subjects at the three stages of the measurements (Pre, Post, and Post II). Accordingly to ANOVA F-test should be followed by the Post-Hoc LSD method to identify which group has the significant differences.
In the following table, class I results shows that Pre-treatment is significantly different from Post treatment and Post II.
6. IV. Discussion
This study was conducted to assess the responses of serum Triglycerides to a treatment program by using the combination of ultrasound and lymphatic drainage machine in chronic atherosclerotic patients, The results showed that there were significant difference in Serum Triglycerides that is strongly correlated with the reduction of the body fat mass studied earlier in the first part of our research With respect to Dennis Jones and Wang Min [12] with the emergence of lymphatic-specific markers, further characterization of the underlying molecular mechanisms for lymph angiogenesis may provide a therapeutic avenue for selective inhibition of lymphatic vessels in diseases such as cancer. On the other hand, stimulation of lymph angiogenesis may be beneficial in diseases of lymphatic insufficiency. Additional study of lymphatic vessel regulation will yield further insight into recent implications of their contribution to transplant rejection, obesity, hypertension, and other metabolic and inflammatory disorders.
Results of this study agreed also with Dennis Jones and Wang Min [12] who stated implications of lymphatic stimulation on obesity, hypertension, and other metabolic and inflammatory disorders. As Lymphatic drainage, techniques improved the level of Triglycerides and Fat mass in chronic atherosclerotic cases. The Impact of Low Frequency Ultrasound and Lymphatic Drainage on Triglycerides Moreover, Palumbo P1 et. al. [13] effects of a new low frequency, high intensity ultrasound technology on human adipose tissue ex vivo were studied. In particular, they investigated the effects of both external and surgical ultrasound-irradiation, in our experimental conditions, both transcutaneous and surgical ultrasound exposure caused a significant weight loss and fat release. This effect was more relevant when the ultrasound intensity was set at 100 % (~2.5 W/cm², for external device; ~19-21 W/cm2, for surgical device) compared to 70 % (~1.8 W/cm² for external device; ~13-14 W/cm2 for surgical device), the effectiveness of ultrasound was much higher when the tissue samples were previously infiltrated with saline buffer, in accordance with the knowledge that ultrasonic waves in aqueous solution better propagate with a consequently more efficient cavitation process. On the other hand, the overall effects of ultrasound irradiation did not appear immediately after treatment but persisted over time, being significantly more relevant at 18 h from the end of ultrasound irradiation. and a significant increase mainly of triglycerides and cholesterol.
The data obtained in our study revealed statistical significance changes in fat mass and the significant improvement (reduction) in the Total blood serum triglycerides for the group A (Class I) and, group B class II groups at the three stages of the measurements (Pre, Post, and Post II). revealed that the combination of lymphatic drainage technique with the low frequency ultrasound reduce the Triglycerides rather than using the low frequency ultrasound only and revealed that there is a positive significant correlation between the reduction of fat mass post-treatment and the reduction of the total body Triglycerides.
This also was consistence with Katsunori Nonogakia et. al. [14], they examined the effects of lowfrequency and low-intensity ultrasound (800 kHz, 2mW/ cm2), Subjects underwent ultrasound irradiation applied to the forearm for 30 min at 800 kHz and 2 mW/cm2 with 100% duty, or placebo irradiation. After treatment for 30 min, BP and pulse rate were again measured using a BP monitoring system, There were no significant differences in age, BMI, serum high-density lipoprotein-cholesterol (HDL-c), low-density lipoprotein-cholesterol (LDL-c), triglyceride (TG), high sensitive-C-reactive protein (hs-CRP), fasting plasma glucose (FPG), HbA1c, systolic and diastolic BP, pulse rate, pulse pressure, CO, TPR, or CI between the placebo controls and ultrasound treatment group Systolic and diastolic BP, pulse rate, pulse pressure, CO, and CI in the ultrasound treatment group, however, were significantly lower than the baseline values in subjects with hypertension, and lower than those of placebo controls.
The present study relayed on objective method of assessment as body composition analysis and Triglycerides evaluation which is considered one of the objective methods that increase the reliability and validity of the study. Results show reduction in Triglycerides that can improve many cardiac cases complications as hyper tension.
7. V. Conclusion
Low frequency ultrasound plus lymphatic drainage technique can be considered a safe and well tolerated method with no life threatening side effects. LFUS plus LD technique improves the blood serum triglycerides fat mass, fat free mass, body water composition, in different types of cardiac obese patients.
Low frequency ultrasound plus lymphatic drainage as a technique could be used as an alternative to conventional exercise and alternative to many obesity surgery as Liposuction surgery and thus provide an opportunity to improve the quality of obese cardiac patient as many obesity surgery have a lot of hazards and sides effect that may affect the patient especially those with cardiac conditions, and that result could be achieved with the usage of LFUS plus LD technique in order to reduce the blood serum triglycerides, fat cells size and even destruction of adiposities with acceptable penetration and get rid of that cells out of the body preventing hazards and complication as thrombosis and many cardiovascular complicated that can be a result of high blood serum triglycerides and high total body fat mass.
8. VI. Acknowledgments

![Fig. (2) : Adipocyte tissueHigh fat masses especially abdominal obesity is associated with an accelerated atherosclerosis, atherogenic blood triglycerides and other compartments of lipid profile, elevated platelet counts in females with chronic inflammation and increased rates of cardiovascular death[6,7].](https://medicalresearchjournal.org/index.php/GJMR/article/download/1040/version/100588/3-The-Impact-of-Low-Frequency_html/9904/image-3.png)
![Fig. (3) : Abnormal adipose tissue and atherosclerosis [6,7].](https://medicalresearchjournal.org/index.php/GJMR/article/download/1040/version/100588/3-The-Impact-of-Low-Frequency_html/9905/image-4.png)
![Fig. (5) : Diffusion of nutrients and waste products between capillaries and cells [9]. While lymph is in many instances, a fluid rich in emulsified lipids, it is interesting to note that fat deposition has a tendency to develop first along lymphatic structures, as it very clearly occurs around mesenteric lymphatics and lymph nodes (Figure (1)).Moreover, nearly all lymph nodes are embedded in adipose tissue and most peripheral adipose depots contain one or more lymph nodes as well.44. However, whether there is a causal relationship between lipid content in the lymph and fat deposition is not known[10].What seems to become clear, however, is that lymph stasis and ? or fluid leakage from lymphatic vessels may promote fat accumulation.45 In our experience, when intestinal lymphatic drainage was interrupted by heat cauterization of guinea pig mesenteric vessels, an obvious increase in mesenteric](https://medicalresearchjournal.org/index.php/GJMR/article/download/1040/version/100588/3-The-Impact-of-Low-Frequency_html/9906/image-5.png)
![Fig. (6) : Proposed working model for the interactions between lymphatic, fat and inflammation[11].](https://medicalresearchjournal.org/index.php/GJMR/article/download/1040/version/100588/3-The-Impact-of-Low-Frequency_html/9907/image-6.png)






| Variable | Groups | Mean ± SD | median | Max -Min | t-value | p-value |
| Age (years) | Class I Class II | 46 ± 3.77 45 ± 3.01 | 46 45.5 | 40 -50 40 -50 | 0.56 | 0.889 NS |
| Weight (Kg) | Class I Class II | 98.5 ± 6.67 110.5 ± 5.55 | 90 114 | 80 -100 110 -120 | 1.011 | 0.765 NS |
| Height (cm) | Class I Class II | 158 ± 5.06 155 ± 4.44 | 155 160 | 150 -160 155 -165 | 1.209 | 0.433 NS |
| BMI (kg/m 2 ) | Class I Class II | 38. 3 ± 1.98 44.5± 3.22 | 37 47 | 35 -39.9 > 40 | 0.97 | 0.766 NS |
| Fig. (13) : The mean values within the two groups | ||||||
| b) Total Body Triglycerides | ||||||
| Mean ± SD | Year 2 015 | ||||||||||
| 25 | |||||||||||
| 38.3 Class I BMI (kg/m2) 44.5 Class II | 98.5 Class I Weight (Kg) 110.8 Class II Demographics 155 Class I Height (cm) 158 Class II | 46 Class I Age (years) 45 Class II | Mean values | Volume XV Issue VI Version I | |||||||
| D D D D ) K | |||||||||||
| ( | |||||||||||
| Medical Research | |||||||||||
| Class I | Total Body Triglycerides Pre treatment Post treatment Post II treatment | Mean ± SD 267.78 ± 34.34 Between Groups 245.01 ± 32.79 Within Groups 240 ± 32.49 Total | Sum of Squares 8767.492 62900.358 71667.850 | ANOVA Table DF Mean Square 2 4383.746 57 1103.515 59 | F 3.973 | Sig .024 | Global Journal of | ||||
| Sum of Squares | DF | Mean Square | F | Sig | |||||||
| Class II | Pre treatment Post treatment | 300.29 ± 66.12 Between Groups Groups 268.39 ± 57.22 Within | 15220.133 125999.91 | 2 57 | 7610.0665 2210.5248 | 3.443 | .038 | ||||
| Post II treatment | 264.89 ± 61.15 | Total | 141220.05 | 59 | |||||||
| © 2015 Global Journals Inc. (US) | |||||||||||
| Variable | Mean Difference Significance | |
| Total Body Triglycerides | ||
| Pre, Post | 22.765 * | (0.034) S |
| Pre, Post II | 22.78 * | (0.011) S |
| Post, Post II | 5.015 | (0.635) NS |
| Table (4) : The mean value of the three measurement of Total body Triglycerides | ||
| Variable | Mean Difference | Significance |
| Total Body Triglycerides | ||
| Pre, Post | 31.9 | (0.098) NS |
| Pre, Post II | 25.049 | (0.029) S |
| Post, Post II | 3.5 | (0.854) NS |