1. Computed Tomography Examination Reveals
Brain Lesions in Guangzhou AIDS Patients Abstract-Cranial computed tomography (CT) plays an important role in the diagnosis of AIDS. However, our understanding of the CT scan images on the diagnosis or evaluating treatment results has not yet been completed. In this study, we conducted an investigation on the usefulness of cranial CT examination in diagnosing HIV patients. Among them, 34 AIDS patients tested positive for brain lesions indicated by cranial CT scan examination. Patients who had AIDS with brain lesions were primarily diagnosed with tuberculous meningitis (TBM), HIV encephalitis (HIVE), cerebral toxoplasmosis (CT) and cryptococcal meningitis (CM). Furthermore, we thoroughly compared the characteristics of various brain lesions in CT images so that it could be helpful for future diagnoses and treatment evaluations of AIDS with brain lesions. Additionally, we demonstrated that a count of less than 50 CD4 + T lymphocytes primarily occurred in the TBM and HIVE groups, thus resulting in higher mortality.
Keywords: AIDS brain lesions, CT scan, tuberculous meningitis, HIV encephalitis, cerebral toxoplasmosis and cryptococcal meningitis. tuberculous meningitis often relies on image features supplied by CT and MR (magnetic resonance) scans; however, it is desirable if a histological examination is available. An operation is required if there is hydrocephalus associated with TBM 7,8 . HIV encephalitis (HIVE) refers to a complex of neuropathological alterations induced by the infiltration of HIV-infected macrophages in the early stages of HIV infection9, 10. It should be noted that antiretroviral therapy (HAART) has quickly altered HIV related neuropathology and neurological manifestations, which could lead to confusion in the treatment of AIDS 9 . Cryptococcal meningitis (CM) presents in brain lesions of AIDS patients because cryptococcus neoformans tend to be present in cerebrospinal fluid. The manifestations of cryptococcal meningitis are characterized by nonspecific symptoms, such as headache, fever, nausea, or altered mental state/behaviour. To confirm the CM diagnosis, a lumbar puncture appears to be vital 11 . Cerebral toxoplasmosis (CT) is one of the most frequent pathogenies that causes brain lesion complication in AIDS patients, especially in developing countries. CT is fatal if not treated properly, although there is possibility for complete recovery as long as the patient is treated legitimately 12,13 .
To diagnose the neurological complications of AIDS, the imaging data supplied by computed tomography (CT) and magnetic resonance (MR) are indispensable. The CT scan is more useful in the diagnosis and evaluation of focal brain lesions, particularly when a MRI facility is not available in underequipped hospitals. For example, a CT scan is able to specifically diagnose cerebral toxoplasmosis in approximately 80% of cases 14 . The accumulating evidence indicates that by mastering the characteristics of the neurological complications of AIDS in CT scans, we can further diagnose these complications and evaluate treatment results. In this study, we performed an investigation of 35 CT scan images of AIDS patients with neurological complications at the 8th Guangzhou People's Hospital.
2. II. Materials and Methods
a) Patients General: From 2004 to 2009, 65 AIDS patients were diagnosed using clinical and laboratory examinations at the 8 th Guangzhou People's Hospital. Among the 65 I. Introduction cquired immune deficiency syndrome (AIDS) is caused by an infection of the human immunodeficiency virus (HIV); hence, it is also known as HIV disease/infection 1,2 . Since being discovered, AIDS has caused the deaths of millions of people's deaths all over the world. Unfortunately, AIDS is far from stable in the world 3,4 . In fact, AIDS itself does not cause death; it interferes dramatically with the human immune system because of the progression of the infection, and it causes HIV-infected people to be considerably more susceptible to common infections, thus enhancing mortality in such conditions 5 .
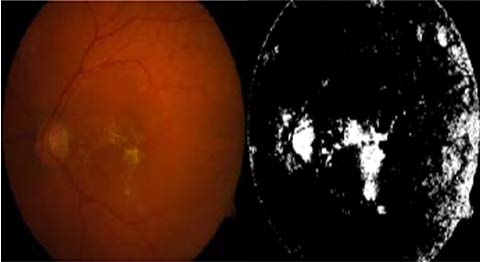
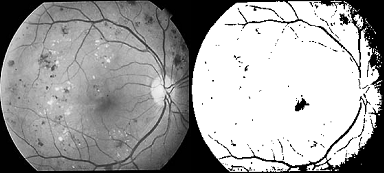
The human immunodeficiency virus and acquired immunodeficiency syndrome can result in several types of complications in the central or peripheral nervous system, which comprise nearly 15 to 40 percent of all AIDS or HIV complications 6 . Tuberculous meningitis (TBM) is one of two brain tuberculosis manifestations. The diagnoses of A Ming-ya Zhang 1 # , Meng Liu 2 # , Hui Zhao The 65 patients suffering from AIDS, proven by their clinical and laboratory examination results, were examined using computed tomography (CT) scan at the 8th Guangzhou People's Hospital from 2004 to 2009. Among the 65 AIDS patients, 45 patients are male (69.2%) and 20 patients are female (31.8%). The patients range in age from 11 to 65 years old, and the average age is 39.3 years old (Table 1). and the incidence of these complications were 35.4% (n=23/65) in TBM, 29.2% (n=19/65) in HIVE, 16.9% (n=11/65) in CT and 18.5% (n=12/65) in CM (Figure 1A). Among the same 65 patients who had been diagnosed with AIDS, numerous brain lesions could be seen in the CT scans of 34 patients. They will be denoted as brain lesion positive in the remainder of this report. These brain lesions included low density foci, local mess effect, ventricle extension, hydrocephaly and encephalatrophy, as illustrated in Figure 2A-D. We determined that the CT scan revealed that 53.3% (n=34/65) of the AIDS patients had brain lesions whereas 47.7% (n=31/65) of the patients did not (Figure 1B). In the CT-indicated positive brain lesion cases, there were 50.0% (n=17/34) HIV+TBM, 23.5% (n=8/34) HIVE, 14.7% (n=5/34) HIV+CT and 11.8% (n=4/34) HIV+CM (Figure 1C). Additionally, low density foci was the most predominant syndrome observed in CT scans for patients with AIDS combined with tuberculous meningitis (TBM) (Figure 1A1). Encephalatrophy was the most apparent syndrome observed in CT scans for patients with AIDS combined with encephalitis (HIVE) (Figure 1B1). Furthermore, encephalatrophy was observed relatively more often in CT scans compared to other syndromes in AIDS combined with cryptococcal meningitis (CM) (Figure 1C1). Low density foci and local mess effect were more common syndromes compared to others in AIDS combined with cerebral toxoplasmosis (CT) (Figure 1D1).
Furthermore, we conducted a questionnaire survey on the personal lifestyle of the 34 AIDS patients with CT-indicated brain lesions. Among these patients, 12 visited prostitutes (35.5%), 10 abused drugs (29.4%), 3 possessed multiple sexual partners (8.8%), 4 patients' spouses suffered from AIDS (11.8%), 2 visited prostitutes and abused drugs (5.9%), 2 visited prostitutes and had blood transfusions (5.9%), and 1 abused drugs and had blood transfusions (2.9%) (Table 2).
The CD4 + T lymphocyte numbers were counted in the four AIDS complications (TBM, HIVE, CM and CT) (Table 3), in which a CD4 + T lymphocyte count of less suggesting that CD4 + T lymphocyte numbers dramatically reduced after the AIDS infection was combined with these complications. e complications might increase the death rate of the AIDS patients. Here, we demonstrate that the highest mortality of AIDS patients with those complications occurred in the TBM group (Table 4).
3. IV. Discussion
Neurological complications account for approximately 40-80% of patients with the human immunodeficiency virus (HIV) infection, especially at a higher frequency in the late stages of severe acquired immune deficiency syndrome (AIDS) 16,17 . To diagnose AIDS-related brain complications, physicians typically use brain imaging information, including internal bleeding, white matter irregularities, and other brain abnormalities based on the patients' medical history and laboratory examination. Furthermore, the diagnosis can be made by combining the general neurological exam to assess various nervous system functions with the brain imaging data, which are primarily supplied by CT and MRI scans. Furthermore, the majority of brain image information is obtained through CT examination due to the expensive costs of MRI examinations in most counties. Thus, precise and thorough CT scans for AIDS-related brain complications are absolutely indispensable. In this study, we conducted cranial CT scans for 65 AIDS patients who visited doctors from 2004 to 2009 at the 8th Guangzhou People's Hospital. A cardinal CT scan revealed that 34 AIDS patients had various brain complications among the 65 patients. Although there were a few differences in the patients' gender and age, we did not determine any significant impact of gender and age difference on the CT scan The combination of AIDS with thes images of AIDS-related brain complications (Table-1). However, the positive CT scan AIDS complications in epidemiological statistics indicated that 35% of patients had a history of visiting prostitutes, and 29% of patients had a history of drug abuse among the positive CT scan cases, suggesting that visiting prostitutes or abusing drugs certainly enhanced the risk of having AIDS brain complications (Table -2). Clearly, we could also see other factors, such as multiple sexual partners and spouses with AIDS, contribute to AIDS related brain complications.
Out of 65 AIDS patients, the percentages of tuberculous meningitis (TBM), cryptococcal meningitis, cerebral toxoplasmosis (CT) and HIV encephalitis were 35.4%, 18.5%, 16.9% and 29.5%, respectively. Furthermore, the percentages of the percentages of tuberculous meningitis (TBM), cryptococcal meningitis, cerebral toxoplasmosis (CT) and HIV encephalitis became 50.0%, 11.8%, 14.7% and 23.5%, respectively in the 53% of CT scan-indicated AIDS-related brain complications, thus demonstrating that AIDS with tuberculous meningitis (HIV+TBM) accounted for half of the brain complications (Fig. 1). This observation is similar to reports by other authors18. It should be noted that AIDS with brain lesions could present as various clinical manifestations or multiple nervous system manifestations simultaneously, or one clinical manifestation could be derived from different pathogenesis. The primary cause for AIDS patients in later stages to see doctors in this study was because of neurological symptoms induced by AIDS-related brain lesions. There are different image characteristics for various AIDS-related brain lesions in CT scans. Additionally, these image features in the CT scan could be useful for diagnosing different AIDS-related brain lesions. For example, low density foci in a tuberculous meningitis (TBM) CT scan indicates an enlarged brain ventricle, hydrocephaly and encephalatrophy. The CT scan images of HIVE encephalitis (HIVE) indicate the presence of broadening subarachnoid space and bilateral ventriculomegaly. The CT scan images of cryptococcal meningitis (CM) present a significant enhancement of bilateral cerebral hemisphere meninx intensity. Furthermore, more low density foci with adjacent oedema and local mess effect appear in CT scan images of cerebral toxoplasmosis (CT).
Additionally, we determined that the CD4+ T lymphocyte count, one indicator for evaluating HIV infection and treatment effect, dramatically dropped (<50) in the TBM and HIVE groups (Table-3). Similarly, a higher mortality of patients who had AIDS with brain lesions could be found in the TBM and HIVE groups, suggesting that it is noteworthy that our physicians should pay more attention to the progress of AIDS with various brain lesions because they could result in a risk to human life. Clearly, a more precise combination of clinical syndromes and CT scan imaging is required in the future to explore the correlation of the types of AIDS brain diseases and their progress.
4. Conflicts of interest
The authors declare that there are no conflicts of interest.

| b) Diagnosis | |||||
| AIDS diagnosis: AIDS could be diagnosed if the patients | |||||
| had epidemiological history (Table 2), HIV positive | |||||
| results in laboratory examination, and any one of the | |||||
| following: fever for more than one month without specific | |||||
| reason, chronic diarrhoea (>3 times/day) for more than | |||||
| one month, over 10% weight loss within half a year, | |||||
| repeated | oral | candidiasis, | repeated | herpes | |
| simplex/herpes zoster virus infection, pneumocystis | |||||
| pneumonia, repeated bacterial pneumonia, active | |||||
| tuberculosis/mycobacterium tuberculosis, deep fungal | |||||
| infection, occupancy lesions in the central nervous | |||||
| system, middle-age dementia, active cytomegalovirus | |||||
| infection, | toxoplasma | cerebropathy, | penicillium | ||
| infection, repeated sepsis and Kaposi's sarcoma in the | |||||
| skin or viscera. | |||||
| AIDS complication diagnosis: The diagnosis of | |||||
| tuberculous meningitis (TBM), HIV encephalitis (HIVE), | |||||
| cryptococcal | meningitis | (CM) | and | cerebral | |
| toxoplasmosis (CT) was followed by the respective | |||||
| standards of the Chinese Medical Association Branch of | |||||
| Infection Diseases in 200415. | |||||