1. I. Introduction
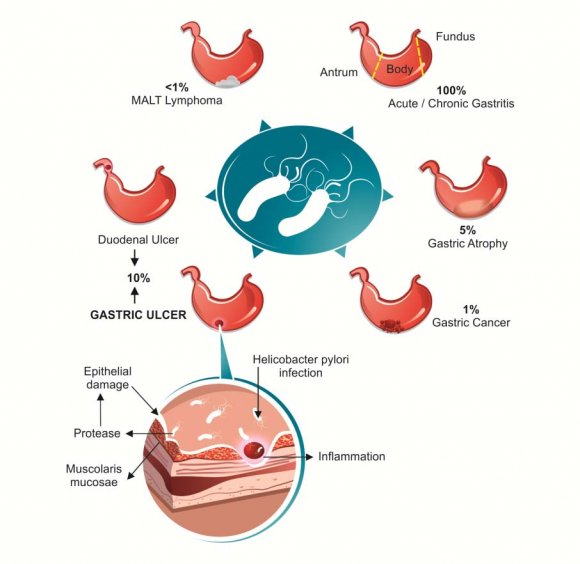
elicobacter pylorus (H. pylori) is a microbial species that specifically colonizes the gastric epithelium. Helicobacter pylori, is a gramnegative, spiral bacterium situated on the epithelial surface of the stomach. It is thought to be the most common bacterial infection worldwide. Virtually, all persons infected by this organism develop gastritis, a signature feature of which is the capacity to persist for decades leading to chronic inflammation of the underlying mucosa. It has been recognized to be associated with increased risk of chronicgastritis, peptic ulcer disease (PUD) (gastric and duodenal),gastric mucosal-associated lymphoid tissue (MALT) lymphoma, gastric adenocarcinoma, World Health Organisation (WHO) has described H. pylori as a class 1carcinogen for gastric carcinoma. H. pylori infection also induces insulin resistance and has been defined as a predisposing factor toT2D development. Gastric and fecal microbiota may have been changed in H. pyloriinfected persons and mice to promote gastric inflammation and specific diseases [1].
Figure 1 : A pictorial representation of the diseases involving H. pylori Although the incidence varies by geographic location and socioeconomic conditions, H. pylori remains one of the most common bacterial infections in the world [2]. Therefore this review aims to find the most prevalent treatment options throughout world in order to eliminate H. pylori.
2. II. Antimicrobial Resistance
The main reason behind failure of treatment is antibiotic resistance. The prevalence of antimicrobial resistance has been found to have regional variance both within countries and outside countries. Studies done in India found that drug resistance in H. pylori was more for metronidazole, tinidazole and clarithromycin [36]. Clarithromycin resistance was also found to be prevalent in many western countries like USA, Canada, Northern, Southern and Eastern Europe [4]. The high prevalence of resistance in the developing countries compared to the industrialised countries is the high rate of antibiotic misuse. Metronidazole is more commonly used in developing countries for the treatment of parasitic infections whereas in developed countries it is more frequently used for dental and gynaecological infections (53). Patients who had had a failed case of H. pylori eradication have been found to be more prone to Since there has been tremendous decline in the cure rate of H. pylori hence sequential therapy was introduced. The sequential therapy in which PPI plus amoxicillin are given for 5 days followed by PPI plus clarithromycin and tinidazole also for 5 days has been found to have eradication rates close to or greater than 90%. In a number of Italian studies this sequential therapy has proved to be superior than the standard triple therapy in eradicating both susceptible and resistant H. pylori strains [8]. The incidence of side-effects was similar with both regimes in these trials. This treatment regimen appeared to overcome clarithromycin resistance. [9] d) First Line Treatment
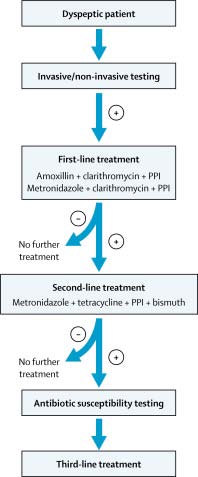
For over a decade the proton pump inhibitor (PPI) -based triple therapy has been used as the first line treatment of choice [10]. The currently approved regimen i.e. (a triple therapy consisting of a proton pump inhibitor, amoxicillin and clarithromycin) has been recommended by the European Helicobacter Study Group [11]. The currently approved regimen now been proven to be relatively ineffective because of the high rate of clarithromycin resistance [12][13][14][15][16]. In many countries this therapy has been considered to be obsolete but since this is the only approved therapy by the government insurance the doctors are still in a dilemma. In the United States four drugs combinations therapy has been used (e.g., 14 day therapy with a proton pump inhibitor, clarithromycin, metronidazole, and amoxicillin or concomitant therapy which is effective except in the presence of clarithromycin-metronidazole dual resistance) or the combination of a bismuth, tetracycline, metronidazole and a proton pump inhibitor which is generally effective despite metronidazole resistance provided it is given a full dose and for 14 days [17,18]. The combination of a high dose proton pump inhibitor and amoxicillin such as 20 mg of rabeprazole and 500 to 750 mg of amoxicillin every 6 hours for 14 days appears to be effective in Asia [19].
No single therapy can be recommended for any area as there are wide variations in the resistance patterns in different parts of the world.
3. Factors influencing outcome:
Treatment:
Strains: Patients:
Increasing the dose of clarithromycin to 1-1.5 mg per day improves cure rates
Resistance of H.pylori to antimicrobial agents.
Depending on geographical region of patients.
The optimal duration of treatment has been found that better cure rates have been found for longer treatment duration.
Strain type.
Patient compliance.
Since so many factors has to be considered, therefore it is very essential to have an organized program to identify the resistance pattern in order to define highly effective regimes.
4. e) Quadruple
Bismuth quadruple therapy entails: bismuth 525 mg four times daily, metronidazole 250 mg four times daily, tetracycline 500 mg four times daily and a standard dose PPI for a total of 7-14 days. On seeing there ported eradication rate of 87%, some authors advocate bismuth based quadruple therapy as first line therapy for H pylori [20][21][22]. In areas of high clarithromycin resistance (> 15 percent) or in patients with a documented penicillin allergy the clinicians may consider Bismuth based quadruple therapy as first line treatment. [23,24]. The side effect profile of standard triple therapy versus quadruple therapy is almost equivalent as the overall adverse event rate in the quadruple therapy treatment arm was 58.5% compared to 59.0% in the triple therapy arm [25,26]. Symptoms included: diarrhea, dyspepsia, nausea, abdominal pain, and taste perversion, changes in stool colour or firmness and headache. f) Second-Line Therapy H. pylori may develop resistance to the prescribed antibiotics used for the first-line therapy. The resistance may be acquired by acquisition and recombination of genes from other bacteria and chromosomic mutations [27,28]. Clarithromycin and Metronidazole appear to be the two antibiotics noted for resistance and most of H. pylori isolates after two eradication failures are resistant to the two drugs [29]. Subsequently, quadruple therapy which consists of PPI, bismuth, metronidazole and tetracycline is a recommended alternative to first-line treatment, which may be advocated in areas of high antibiotic resistance.
In any case if bismuth is not available, second-line therapy may be with PPI-based triple therapy. [10] g) Third-Line (Rescue/Salvage) Therapy
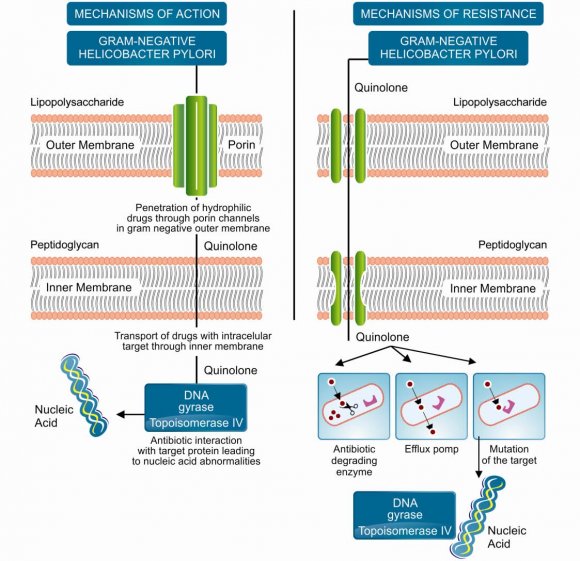
On multiple (at least two) treatment failures with different regimes the third line therapy is applied. Ideally, it would be chosen based on the results of antimicrobial susceptibility testing. Since it was noted that most of H. pylori isolates after two eradication failures are resistant to metronidazole and clarithromycin therefore, has been recommended to exclude the two drugs from the third-linetherapy. As a result, the third-line therapy is now being applied in some countries. These third-line therapies are the new emerging therapies. [8] Volume Concomitant therapy entails: Standard dose PPI, Amoxicillin 1000mg twice daily, Clarithromycin 50m mg twice daily and Metronidazole500 mg twice daily for 10-14 days. In terms of eradication it is similar to sequential therapy with an eradication rate of 94% and maybe a simple rregimen when compared to sequential therapy as all antibiotics are give nat once. A randomized trial comparing sequential and concomitant therapy, demonstrated comparable eradication rates (92.3% versus 93%,respectively) and similar adverse event rates (30.7% versus 26.9%).A regimen consisting of: esomeprazole and amoxicillin for seven days then esomeprazole, amoxicillin, clarithromycin, and metronidazole for 7 seven days (sequential-concomitant hybrid therapy) generated a99.1% eradication rate in 117 patients [2]. i) Emerging Therapies i. Fluroquinolone based therapies Levofloxacin-based triple therapies are now becoming the second-line treatment of choice in some European countries. It has proven very effective in the treatment of H. pylori infection in a study carried out in Italy. In a comparative study in Italy, the eradication rate achieved with levofloxacin-based triple therapy as a first-linetreatment was significantly higher than that with standard therapies. Levofloxacin has been advocated for use insecond-and third-line "rescue" regimens. Levofloxacin may thus represent a reasonable treatment regimen in the setting of Clarithromycin resistance [8] ii. Lactoferrin Lactoferrin is a natural antibiotic which is found in bovine milk. It has been found to be bacteriostatic to H. pylori both in vivo and in vitro. It is a milk protein that binds iron and its addition to the regular treatment regimen for H. pylori may improve eradication rates.
Studies have been carried out to determine its use in combination with PPI and other antibiotics with varying efficacies. This modality of treatment has not been universally accepted [8]. Korean cohort [30]. Further multi-centred studies may be required in other countries.
5. III. Conclusion
Despite the introduction of various treatment regimens, H. pylori infection is still a major problem of concern. Though the clinicians have many different treatment regimens within them but standard PPI based triple therapy and bismuth based quadruple therapy remain in first line as the eradication remain relatively high (70-80%). The increased resistance of drugs and non compliance, due to complexity of regime and associated side effects has led to the investigation of many other therapeutic options which is necessary for the complete eradication of H. pylori. Hence from this review we can conclude that further many more trials are necessary to get a complete eradication of H. pylori.
6. IV. Future Treatment Module
The next generation of H.pylori therapeutic regimens should be simpler, novel and specific. There are some novel approaches available to achieve this goal, such as-1) Development of therapeutic vaccine 2) Genome based drug discovery 3) Pathogen -host tissue adhesion inhibitor 4) Novel site specific drug delivery at specific site of H. pylori infection.
Although combination therapies have been found to have high rates of eradication, therapies that would be preferred are the ones which use a low dose of single drug with a short duration treatment and without any adverse effect.