1.
MRI Study of the Psoas Major Muscle and its Attachments to the Lumbar Intervertebral Discs: Can a Partial or Absent Attachment of the Psoas to the Disc Trigger Herniation of the Disc?
Abstract-Background: The Psoas Major muscle attaches to the discs from its origin until the level of L4-L5 disc. It rarely attaches to the L5-S1 disc, and the absence of attachment of the psoas to the L4-L5 disc is frequently seen. Likewise, disc herniation occurs more often at these two lower lumbar discs L4-L5 and L5-S1. Hypothetically, by attaching the disc, the psoas may provide support to the fibrous annulus and prevent herniation of the nucleus pulposus. That may explain the higher incidence of herniation of the lower lumbar discs where the psoas attachment is frequently absent.
Purpose: 1) To search for the location of disc herniation in the lumbar spine, 2) To determine whether the site of the disc herniation coincides with a partial or a total absence of psoas major (PM) attachment to the disc.
Materials and Methods: One hundred and seventy-five magnetic resonance imaging (MRI) lumbar spine examinations from Rashid Hospital, Dubai, UAE were reviewed. There were 89 females, and 86 males, twenty-four East Asians and 151 Arabs, mean age 53.2 (range 21-75) years. The participants were selected by one physician. The inclusion criteria were presence of low back pain, paresthesia, radiculopathy. All selected participants underwent MRI spine examinations. All MRI examinations were performed with the same sequences. The MRI images were read by three Radiologists who were blinded to the clinical examination results such as level of dermatomes and side of symptoms. The location and prevalence of nonattachment of the psoas to the three lower discs were assessed. The association of psoas nonattachment to the disc and disc herniation was calculated using the Pearson Chi Square test with 95% confidence interval (CI), and two-sided p value <0.05 for statistical significance.
Results: At the L5-S1 disc, 16 (9.1%) patients presented with partial attachment of the PM; and 75% of them had disc herniation. One hundred and fifty-nine (90.8%) patients had nonattachment of the PM to the L5-S1 disc; amongst them, 60% suffered from disc herniation. At the L4-L5 disc, partial attachment and nonattachment of the PM to the disc was detected in 77 (44%) patients. Disc herniation was seen in 45 (79.2%) of them. At L3-L4 disc, 12 (6.8 %) patients presented with partial attachment of the PM to the disc. Disc herniation was present in 58.3% of them. The PM's partial attachment and nonattachment to the disc was more common in females at all three disc levels, the highest incidence being at L4-5 level in 60.7% of females compared to 26.7 % of males, p= .0001.
There was a higher prevalence of disc herniation at L5-S1 in the older age group (76.1%), compared with the younger age group (52.4%), p=.003. The presence of disc herniation associated with nonattachment of the PM muscle to the disc was higher at L4-L5 disc among the younger age group (47.6%) compared with the older age group (23.9%), p=0.003 Conclusions: The partial attachment or nonattachment of the psoas muscle to the lumbar disc may trigger disc herniation with a higher incidence in females and in the younger age group.
2. I. Introduction
natomically, the psoas major (PM) muscle attaches to the lumbar intervertebral discs, to the vertebral bodies and to the transverse processes (1). At the discs level the PM adheres to the fibrous annulus on both sides. In most individuals, the muscle connects to the disc at its anterolateral borders, although it may occasionally extend to the posterior border close to the lateral recess (1,2). Anatomical variants such as partial attachment and nonattachment of the PM to the discs exist; although their prevalence is unknown. Previous reports mentioned the frequent absence of attachment of the PM to the L5-S1 disc and the occasional partial attachment to the L4-L5 disc (3).
The attachment of the PM to the lumbar discs remains enigmatic both from a biomechanical standpoint and from a Radiological perspective. Hypothetically, the PM's attachment to the disc provides support to the fibrous annulus and therefore would prevent extrusion of the nucleus pulposus. Likewise, it can be speculated that the lack of attachment or partial attachment of the PM to the lower lumbar discs L3-L4, L4-L5 and L5-S1, can be a contributing factor in the advent of disc herniation or extrusion. This is a hypothetical thought that has not been thoroughly investigated.
In the general population, the higher incidence of herniation occurs at the lower lumbar discs L4-L5 and L5-S1 (4,5), where the nonattachment of the PM muscleis frequent. This can be a cause-effect phenomenon which has not been demonstrated neither biomechanically nor radiologically. The aim of this study is to assess the prevalence of disc herniation in patients with low back pain and search for possible association with the PM muscle's partial attachment or non attachment to the affected disc.
3. II. Materials and Methods
4. a) Selection of participants and collection of clinical data
This is a retrospective study. The material consists of magnetic resonance imaging (MRI) examinations of the lumbar spine performed from October 2015 to April 2016. The images were retrieved from the picture archiving communication system (PACS) of our Institution. All patients were referred to the Radiological Department by their attending physician because of low back pain of variable duration and paresthesia in the lower extremities originated from the three lower lumbar nerve roots.
During the selection of the material, the criteria set to participate in the study included: a) history of low back pain of long or short duration, b) presence of clinical symptoms -paresthesia, motor deficit, or neurological deficit -suggesting presence of lumbar disc herniation, c) a complete MRI examination of the lumbar spine which included the three lower lumbar discs in axial and sagittal planes. The patients with primary or secondary malignancies, history of trauma, congenital disease affecting the musculoskeletal system such as muscular dystrophy, previous spinal surgery with hardware, history of infection (spondylodiscitis) with destruction of the disc and endplates, were excluded from the study. The demographic data (age, gender, ethnicity), clinical and radiological data of each participant were collected from the electronic Archive system of the same Institution. One hundred and seventy-five patients were selected for the study. Their age ranged from 21 to 75 years, with a mean of 53.8 years. They were 89 females, and 86 males. Among them there were twenty-four East Asians and 151 Arabs. All participants underwent MRI examination of the lumbar spine with the same imaging protocol.
5. b) MRI examination of the lumbar, sequences and imaging parameters
All selected MR examinations contained images in sagittal and axial planes with cross-sectional slides of at least the three lower lumbar discs from L3 to S1. The images were obtained from a 1.5 Tesla GE imager. The series of images were acquired with the following sequences: a) turbo spin echo (TSE) T1Weighted (T1W) in sagittal plane, b) TSE T2Win sagittal plane, c) short Tau-Inversion Recovery (STIR) in sagittal plane, and d) TSE T2W in axial plane. With a slice thickness of 3 millimeters, a field of view (FOV)of 200, a matrix of 416x288, the number of signal average (NSA) of 1-3, a repetition time (TR)=T1Wof 580 milliseconds (ms), T2W (4660ms), STIR(2860ms), echo time (TE)=T1W (11.9ms), T2W(82.19ms), STIR(33.92ms), inversion time (IT) =125, echo train (ET) of T1W =3, of T2W=24, of STIR=12, the examination time would not exceed thirty minutes.
6. c) Analysis of MR images and assessment of the PM attachment to the disc
The images were analyzed by two experienced Radiologists, as the decisions were reached by consensus. The results were supervised by two senior Radiologists.
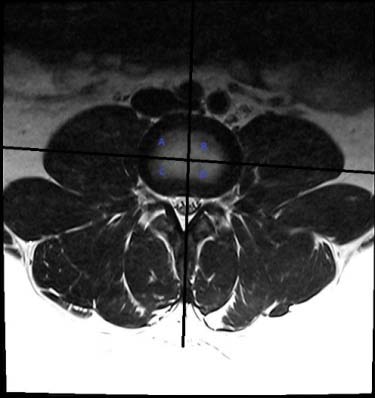
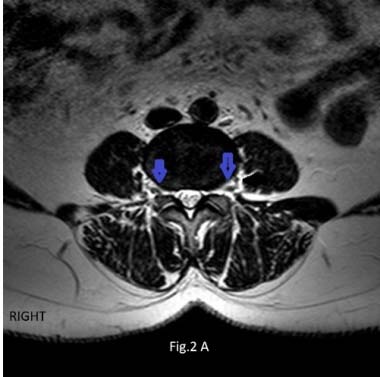
The analytic process was three-fold: a) search for disc herniation in the three lower lumbar discs, with emphasis of its location central or lateral, 2) assess the attachment of the PM muscle to both sides of the disc, and verify if the attachment was present, partial, or absent (nonattachment), and 3) verify whether there was disc herniation and partial or absent attachment of the PM muscle to the same disc. To facilitate the assessment of the PM muscle adherence to the disc's borders, and to correctly locate the herniated disc, the disc's surface was divided into four quadrants of equal size. The four quadrants were obtained by drawing two perpendicular lines at the center of the disc (Figure 1). The quadrants were named: right anterolateral, left anterolateral, right posterior, and left posterior. When the muscle fascicles adhered to the disc in all four quadrants, it was considered as complete attachment (Figure 1). The lack of contact of the PM muscle fascicles with the disc border in one, or two, or three quadrants was defined as partial attachment (Figure 2a). The lack of contact of the PM muscle fascicles to the disc in all four quadrants was defined as total absence of attachment or nonattachment (Figure 2b).
The PM muscle's attachment to the discs were assessed on the TSE T2W axial images. The presence of lumbar disc herniation was assessed at the last three lower lumbar levels, on both sagittal and axial images. The herniation site was defined as: diffuse, right, central, or left. The disc was considered as herniated when it bulged more than 2 mm from the vertebral margin.
For comparison purposes, the population was sub-classified, based on age, into two sub-groups: group I (21-45 years) and group II (46-75 years). There were two other sub-groups based on gender: male and female; and based on ethnicity: East Asians and Arabs. The data were collected on Excel spread sheets prior to statistical analysis.
7. d) Statistical analysis
The data was processed with a SPSS software (IBM) version 20 and different categorical variables were tabulated for frequency and percentages separately. For analyzing the association between two categorical variables we cross tabulated variables and used Pearson Chi Square test to see the significance of association between two variables. With 95% confidence interval (CI), two-sided p value <0.05 was considered statistically significant.
8. III. Results
9. a) Prevalence of disc herniation
Out of 175 patients, disc herniation most frequently occurred at L4-5 levelin 126 (72%). This was followed by L5-S1 level, in 108 (61.7%) patients; and then by L3-L4 level in 87 (49.7%) patients. The most common patterns of disc herniation and their prevalence at the three disc levels L3-L4, L4-L5, and L5-S1 are presented in Table I.
10. b) Prevalence of PM's partial attachment and nonattachment to the discs associated with disc herniation at the three levels
At the L5-S1 disc level, none of the 175 patients presented with a complete PM attachment to the disc. However, 16 (9.1%) patients presented with a partial attachment of the PM muscle to the disc; while 159 (90.8%) patients had nonattachment of the PM muscle to the disc.
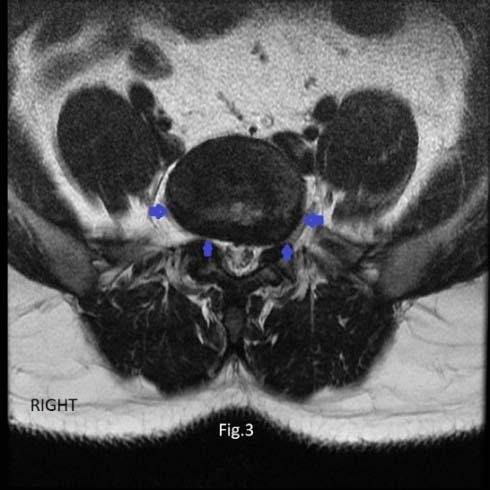
Amongst the 16 patients with PM partial attachment to the disc, 75.0% had disc herniation. From the 159 patients with nonattachment of the PM muscle, 60% suffered from disc herniation (Figure 3). Statistically, the difference in the prevalence of disc herniation in patients with partial attachment and those with nonattachment was insignificant, p=0.371.
At the L4-L5 disc level, there was the highest prevalence of partial attachment and nonattachment of the PM muscle to the disc. It was seen in 77 (44%) patients. Out of the 77 patients with partial and nonattachment, 45 (79.2%) showed disc herniation (Figure 4); compared with 37 (66.3%) patients out of 98 patients with complete psoas attachment and disc herniation, showing a trend of significance, p value = 0.059.
At the L3-L4 disc level, only 12 (6.8 %) patients presented with partial attachment of the PM muscle to the disc. Out of the 12 patients, disc herniation was present in 58.3%, compared with 49.1% patients with complete PM attachment to the disc, which was not statistically significant, P value for Chi Square =.536.
11. c) Prevalence of side (right / left)of PM muscle partial attachment only at the three discs L3-L4, L4-L5 and L5-S1
When the PM partial attachment to the disc was analyzed separately at each disc level, at L5-S1 disc more patients were seen with partial PM attachment to the right side of the disc compared with the left side, 15 (8.5%) and 7 (4%) respectively.
At the L4-5disc, the PM was partially attached in sixty-seven (38.2%) patients on left side of the disc compared with 63(36%) patients where the PM was partially adhered to the right side of the disc (Fig. 4).
At the L3-L4 disc level, eight (4.5%) patients had partial attachment of the PM on the left side of the disc; and 8 (4.5%) patients had partial attachment on the right side of the disc.
12. d) Prevalence of disc herniation and complete PM
attachment to the disc at the three levels At L5-S1 disc level, none of the participants had complete PM attachment to the disc. However, disc herniation was seen in 60.1% of patients with nonattachment of the PM to the disc.
At L4-L5 disc level, disc herniation was observed in 66.3% of patients with complete PM attachment to the disc.
At L3-L4 disc level, disc herniation was seen in 49.1% of patients with bilateral complete PM attachment to the disc.
13. e) Prevalence of disc herniation in the two age groups, genders and ethnic groups
Based on age, the population was divided into subgroups. There were 104 patients in the younger group (age 21-45 years) and seventy-one patients in the older group, (age 46-75 years).
At L5-S1 disc level, disc herniation was detected in 52.4% of the patients from first age group, compared with 76.1% of patients from older age group, being the difference statistically significant, p = .003.
At L4-L5 disc level, among the younger age group of 104 patients, there was a higher prevalence of disc herniation and nonattachment of the PM muscle to the disc, 45 (47.6%) patients compared with 23.9% of patients from the older age group, p value =0.003.
At L3-L4 disc level, the difference in prevalence of disc herniation between the two age groups was less important. The prevalence was 40.2% in the younger population compared with 58.6% in the older population.
When the two gender groups (female and male) were considered, there was a higher prevalence of disc herniation in females compared to males especially at the level of L4-L5 disc, although not significant. The prevalence of disc herniation in the two age groups, genders and the ethnic groups at all three disc levels is shown in Table II.
14. f) Prevalence of partial attachment and nonattachment in the two age groups, the two gender groups and the two ethnic groups
The analysis of the two age groups revealed a higher prevalence of the PM's partial attachment and nonattachment to the discs in the older population. This difference was more accentuated at the two lower discs. At L4-L5 disc, the partial and nonattachment of the PM ( D D D D ) D muscle to the disc was seen in 49.3% in the older group compared to 39.8% in the younger group. At L5-S1 disc, the partial and nonattachment of the PM muscle to the disc was detected in 12.7% in the older group compared to 6.8% in the younger group.
When the two genders groups were considered, the PM' spartial attachment and nonattachment to the disc was more common in females compared to males, at all three disc levels. The incidence was highest at L4-5 level, in 54 (60.7%) females, compared to 23 (26.7 %) males, p= .0001.
Among the 24 participants from East Asia, 12 (50%) of them presented with partial attachment of the PM to the disc at L4-L5, compared with the Arabs. However, among the 151 Arabs, 11 (7.3%) of them had apartial attachment of the PM at the L3-L4 disc compared with a lower incidence among the East Asians.
The prevalence of PM's partial and nonattachment to the discs in the two age groups, gender groups and ethnic groups is presented in Table III. Table II: Prevalence of disc herniation in the two age groups, genders and the ethnic groups at all three disc levels.
15. IV. Discussion
On magnetic resonance (MR) cross-sectional images, the PM muscle emits a moderate signal intensity compared to other muscles. The sagittal images are less useful to evaluate the PM, while the axial slicespermit a fair appreciation of the PM's attachment to the lumbar intervertebral discs and the anatomical variants. In this study, the authors aimed to analyze the relationship between the pattern of attachment and nonattachment of the PM to three lumbar disc and the possible impact on the herniation of the disc.
In previous studies, several conditions such as abnormal posture (6), increased intradiscal pressure (7,8) have been mentioned as causative factors of lumbar disc herniation. The partial attachment or nonattachment of the PM to the disc had not been considered as possible influential factors to disc herniation. Neither the differences in the prevalence of these anatomical variants with regards to demographics have been subject to investigation. Hypothetically, we postulated that individuals with anatomical variations of the PM attachment to the disc may suffer from a higher risk of herniation, assuming the PM's attachment to the disc would provide support to the fibrous annulus and therefore prevent annulus tear and extrusion of the nucleus pulposus.
At the L4-L5 disc, we found the highest prevalence of partial attachment and nonattachment of the PM muscle to the disc in 77 (44%) patients. Of them, 45 (79.2%) suffered with low back pain and disc herniation. This finding pointed toward a possible cause and effect phenomenon that has not been previously considered. In our study, a population of 175 subjects was evaluated. The highest prevalence of disc herniation (72%) was detected at L4-L5 level, which concurred with previous reports (4,5,8).
The PM's nonattachment to the L5-S1 disc has previously been reported (8,9), and considered as anatomically normal, since it occurs in most individuals. In our study, the nonattachment was seen in 159 (90.8%) subjects with a high prevalence of herniation (60% of them). Of the rest -16 (9.1%) subjects-, who presented with PM's partial attachment, 75% had disc herniation. Such high occurrence of disc herniation at the two lower discs and the high prevalence of the PM's partial and nonattachment to the disc may be related.
From the study's results, the demographic factors -age and gender-seemed to have some influence on the advent of disc herniation in individuals with partial or nonattachment of the PM to the disc. We found that a higher frequency of disc herniation at L4-L5 level and L5-S1 level in the younger individuals with partial or nonattachment of the PM to disc. The difference in prevalence was more accentuated at L4-L5 disc, 47.6% versus 23.9% with statistical significance (p=0.003). This further emphasizes the role of muscle attachment pattern in inducing herniation of the disc, with a possible stronger influence among younger subjects.
Also, a significant association between the PM's muscle nonattachment to the disc and disc herniation was found with a higher frequency infemales (60.7%) compared to males (26.7%), especially at the L4-L5 disc. This difference has not been described previously. The selected population was represented by two different Ethnic groups: Eastern Asians (24 subjects) and Arabs (151 subjects). Because of the discrepancy in the numbers (24 versus 151) no significant comparative data could be obtained for the two ethnic groups; which constitutes a limitation of the study.
A study with a larger population with larger diverse ethnic groups may be necessary to better understand the correlation between ethnicity, PM's attachment to the disc and disc herniation. Likewise, the statistical difference between genders and different age groups for PM's attachment to the disc and disc herniationdeserve further investigation. To our knowledge, no previous study had focused on the PM muscle attachment to the disc as a possible contributing factor in disc herniation in relation with demographics.
In conclusion, the PM muscle's partial attachment and nonattachment to the lower lumbar discs may be a triggering factor for initiating disc herniation especially in younger age groups and in females. Further prospective studies with larger population are needed to confirm this hypothesis.


| LEVELS | 21-45 YEARS | 46-75 YEARS | MALES | FEMALES | EAST ASIANS | ARABS |
| L3-L4 | 3.9% | 11.3% | 2.3% | 11.2% | 4.2% | 7.3% |
| L4-L5 | 39.8% | 49.3% | 26.7% | 60.7% | 50.0% | 43.0% |
| L5-S1 | 6.8% | 12.7% | 8.1% | 10.1% | 16.7% | 7.9% |