1. I. Introduction
mphysematous cholecystitis is a severe form of acute cholecystitis characterized by gas production in and around the gallbladder wall caused by gas-forming organisms. It is associated with increased morbidity and mortality. We report a case of emphysematous cholecystitis in 84 years old diabetic man who was successfully treated with percutaneous cholecystostomy. We also review the literature for the role of percutaneous cholecystostomy in the management of the condition.
2. II. Case Report
84-year-old male presented to our emergency department with right upper quadrant abdominal pain of two days duration. He had history of chronic dyspepsia, fat intolerance and recurrent mild right upper quadrant abdominal pain for few years before his presentation. He was known diabetic and hypertensive on medical treatment. He had CAPAG 6 month before admission and he was on regular dose of anticoagulants.
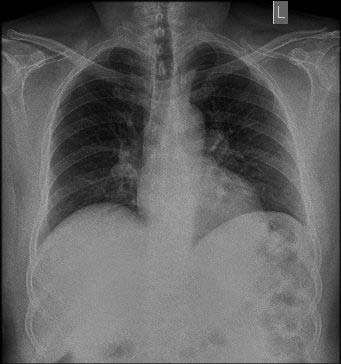
On examination he was febrile with temperature of 38.8c. His blood pressure was (80/40 mmHg), pulse was 120 and respiratory rate was 28/min. His abdomen was slightly distended with remarkable tenderness and rigidity over the right hypochondrium. Murphy's sign was positive. His ECG was normal and his blood gas analysis showed slight metabolic acidosis. His hemoglobin was (13 g/dl). Urea and electrolytes, liver function test and serum amylase were within normal values. His erect chest X Ray excluded free air under the diaphragm (Figure 1). After initial fluid resuscitation he had abdominal CT scan (Figure 2A & B) which showed a distended thickened wall gallbladder containing air within its wall and lumen with air-fluid level. There was also a curvilinear hyper density in relation to the gallbladder wall, with gallbladder wall calcification and pericholecystic fat stranding extending to the region of the hepatic flexure. There was no obvious evidence of gallstones seen and no evidence of intra-or extrahepatic biliary dilatation. The CT scan findings were consistent with non-calculus emphysematous cholecystitis. The patient did well and discharged on the 7 th post cholecystostomy day. The cholecystostomy tube was removed after 6 weeks and he remained symptoms free on follow up for more than a year.
3. E
4. III. Discussion
Emphysematous cholecystitis also known as acute gaseous cholecystitis, aerocholecystitis, pneumocholecystitis, and gas gangrene of the gallbladder, is a severe variant of acute cholecystitis characterized by gas production in and around the gallbladder wall or in the pericholecystic space. (1) The disease was first described by Stolz1 who reported three cases discovered accidentally at autopsy 1901.
(2-3) Pende was the first to record a description of the findings at surgery in 1907. (4) Lobingier reported the first case in the English literature in 1908 (5) and Hegner was the first to make preoperative radiologic diagnosis in 1931. (6) This disease is considered interesting and merits the report of a single case because of its relative rarity, its unusual radiologic and clinicopathologic characteristics and its increased incidence among male diabetics. (7) The disease is relatively rare compared with non-emphysematous cholecystitis. It is common in males with male: female ratio is 7:3. ( 8) It is also more common in older patients with diabetes mellitus than in the general population. (1) Although emphysematous cholecystitis develops in approximately 1% of all cases of acute cholecystitis, this entity is potentially more severe than acute non-emphysematous cholecystitis because in emphysematous cholecystitis gallbladder gangrene is 30 times higher and perforation occurs 5 times more frequently than in acute non-emphysematous cholecystitis (9) together with significantly increased rates of mortality (15-25%). (10) The assumptive pathology of the condition is cystic artery occlusion secondary to inflammation from acute cholecystitis or small vessel atherosclerosis leads to gallbladder wall ischemia and overgrowth of gasproducing bacteria. The bacteria most frequently isolated in these instances include Clostridial species, with Clostridia welchii being the most common. E. coli is isolated with the second most frequency. (10 and 11) Clinical presentation of the condition is similar to acute non-emphysematous cholecystitis, with right upper quadrant pain, low-grade fever, nausea and vomiting. Peritoneal signs include tenderness in the right hypochondrium and positive murphy's sign may be present. A mass in the right upper quadrant may be palpated in half of the patients. (12) Diagnosis depends on the characteristic radiological appearance. On imaging, the condition is diagnosed when there is radiographic demonstration of air in the gallbladder wall in the absence of an abnormal communication with the gastrointestinal tract. (13) Bloom RA, et al described the ultrasound spectrum of emphysematous cholecystitis classifying them into 3 stages; in the first stage Gas is present in the gallbladder lumen. There is a dense band of hyperreflective echoes with distal reverberations when the gallbladder is full of gas or a band of reverberations in the gas-filled portion of the gallbladder with the usual signs of cholecystitis in the bile-filled portion when the gallbladder is partially full of gas. In the second stage the gas is present in the gallbladder wall in absence of an area of high reflectivity in the gallbladder wall with reverberations that may change position with patient movements or a bright hyper reflective ring emanating from the entire gallbladder circumference. In the third stage the gas is present in the pericholecystic tissue and is seen inside the gallbladder, within its wall and outside the gallbladder in the surrounding tissues, indicating gangrene and perforation. (14) In some cases, there may be multiple tiny echogenic foci in the gallbladder lumen, arising from the dependent part of the gallbladder and "floating" to the nondependent wall, reminiscent of bubbles rising in a glass of champagne (15,16,17).
Abdominal CT scan is now considered the primary imaging modality to confirm acute emphysematous cholecystitis, as it is the most sensitive and specific imaging modality for identifying gas in the gallbladder lumen or wall. (18,19) CT scan demonstrates emphysematous changes in the gallbladder wall that are diagnostic of this condition and is highly sensitive for tiny bubbles of air which may not be seen on ultrasonography. It can also provide precise information regarding the location and extent of air and fluid collections, such as extension into the pericholecystic tissues and the hepatic ducts. Gas in the peritoneum indicates perforation. (20) Magnetic resonance imaging (MRI) can provide extensive information on intramural necrosis as well as intraluminal gas. Gas in the gallbladder lumen and wall appear as signal void areas. (21) Characteristic MRI findings of emphysematous cholecystitis are numerous floating signal void bubbles in the upper dependent portions of the gallbladder (22).
The traditional management of emphysematous cholecystitis is urgent surgery after fluid resuscitation because of the risk of gangrene and perforation with overall, surgical mortality rates vary from 15% to 25%. (10), However due to recent advances in imaging and interventional radiology percutaneous cholecystostomy is now considered as one of the options of management of the condition especially in high risk patients.
The role of cholecystostomy in the era of laparoscopic surgery is well established for high risk and debilitated patients with an obstructed gallbladder, in whom open operation or laparoscopic interventions associated with high morbidity and mortality. (23) At present, many authors consider percutaneous cholecystostomy is a cost-effective, easy and reliable procedure with low complications and high success rates for high-risk patients with acute calculous cholecystitis, and definitive treatment in patients with acalculous cholecystitis (24)(25)(26)(27)(28)(29).
Although many papers were published in the role of percutaneous cholecystostomy in management of acute non-Emphysematous cholecystitis in seriously ill patients, unfortunately till present, there is no published large-scale studies about the role of percutaneous cholecystostomy in management of condition in seriously ill patients. This most probably due to the rarity of the condition and its sporadic presentations. Most of the published literatures about the condition are occasion case reports.
Slot WB et al (30) reported a case similar to our case reporting successful percutaneous drainage of gallbladder in a male diabetic patient with emphysematous cholecystitis in whom surgery was considered contraindicated because of his poor cardiac status. On the other hand, Safioleas M et al (31) reported 5 cases of Emphysematous cholecystitis, three of them were treated with open cholecystectomy without complication. The remaining two were treated with percutaneous drainage; both of them developed septic musculoskeletal complications. They recommend that surgeons must be aware of musculoskeletal complications of percutaneous trans gallbladder drainage in patients with emphysematous cholecystitis.
5. IV. Summary
Emphysematous cholecystitis is relatively rare life-threatening form of acute cholecystitis caused by gas producing organisms. The clinical picture is similar to that of acute non-emphysematous cholecystitis with early signs of sepsis and rapid progress to gangrene and perforation. Demonstration of air in the gallbladder wall in the absence of an abnormal communication with the gastrointestinal tract in plain abdominal x ray and CT scan is diagnostic. The traditional management of emphysematous cholecystitis is urgent surgery after fluid resuscitation because of the risk of gangrene and perforation; however with the recent advances in the field of intervention radiology, percutaneous cholecystectomy may provide an alternative noninvasive option of treatment especially in high risk patients. With the anticipated difficulty of publication of large scale studies due to rarity of the condition we encourage publication of each single case treated with percutaneous drainage.