1. Introduction
stroke or Cerebrovascular accident (CVA) is defined as an abrupt onset of a neurologic deficit that is attributed to a focal vascular cause. 1 A stroke or Cerebrovascular accident (CVA) is defined as an abrupt onset of a neurologic deficit that is attributed to a focal vascular cause. 2 A stroke or Cerebrovascular accident (CVA) is defined as an abrupt onset of a neurologic deficit that is attributed to a focal vascular cause. 3 Stroke can cause the loss of control over an arm and a leg, people's abilities to care for themselves in simple ways like washing or getting dressed and to undertake taken for granted daily activities like preparing a meal, cleaning or going to the shops are often affected. Even the simplest tasks like brushing teeth, shaving or getting toilet roll out of a dispenser became seemingly unmanageable. 4 Hemiplegia, a paralysis of Author ? ?: e-mail: [email protected] one side of the body, is the classic sign of neurovascular disease of the brain. It is one of many manifestations of neurovascular disease, and it occurs with strokes involving the cerebral hemisphere or brain stem. A stroke, or cerebrovascular accident (CVA), results in a sudden, specific neurological deficit. 5 Clinically, a variety of focal deficits are possible, including changes in the level of consciousness and impairments of sensory, motor, cognitive, perceptual, and language functions. Motor deficits are characterized by hemiplegia or hemiparesis, typically on the side of the body opposite the side of the lesion. The location and extent of brain injury, the amount of collateral blood flow, and early acute care management determine the severity of neurological deficits in an individual patient. Impairments may resolve spontaneously as the brain swelling subsides, generally within 3 weeks. Residual neurological impairments are those that persist longer than 3 weeks and may lead to lasting disability. 6 The large vessel diseases such as: Coronary diseases, Cerebrovascular Diseases and Peripheral Vascular Diseases are the major causes and hypertension, diabetes, smoking, hyperlipidemia are the most common risk factors for Ischemic stroke. Stroke appears to be a preventable disease to a large extent, change in lifestyle is supposed as the major primary prevention strategy. 7 Stroke patients usually presents with a history of a sudden or rapid onset of focal neurological symptoms. Some patients may have a stepwise or gradual worsening or waxing and waning of symptoms. Most patients are alert, although patients with major hemispheric infarctions, basilar occlusion or cerebellar strokes with oedema causing brain stem compression can have a decreased level of consciousness. Headache occurs in approximately 25% of the cases. Nausea and vomiting can occur with stroke in the brain stem or cerebellum. 8 Most typical symptom of stroke is hemiparesis or hemiplegia which ranges from weakness to full paralysis of the body opposite to the side of the lesion in the brain. 9 Majority of stroke patients complain of activity limitations and participation restrictions. 10 Activity limitation consists of limitations in walking, limitations in self-care activities, and limitations in domestic life activities, such as inability to walk independently, dependence on bathing, eating and dressing, as well as in housework activities such as washing, cooking, cleaning, food preparation, shopping, and public transport use. Whereas, participation restrictions include inability to return to previous occupation, decreased social interactions, and inability to participate in religious activities. 11 Walking is the most basic means of human transport in daily life. 12 Because stair climbing is a common activity of daily living, the ability to do it efficiently is important to an individual's quality of life. More demanding than level walking, stair ambulation is performed with ease by healthy individuals; however, it is more difficult to perform for those with decrements in motor function, balance problems, or reduced lowerlimb function. 13 Independent living requires physical mobility beyond walking. Stair negotiation is an important determinant of discharge destination and independence, surpassing walking speed as the single best predictor of community ambulation. Despite this, little is known about the physical demands of stair negotiation in rehabilitation populations such as stroke. 14 Stairs are used frequently in daily life, and differences between stair gaits and at flat surface gaits have been reported. In stair gaits, each step starts from the toes or the sole rather than the heel. Force is required to push the body upward and forward, and control of the body against falls is required when descending stairs. More dynamic effort is required in stair gaits than at surface gaits because an awareness of body balance and lower extremity force is necessary. 12 Stair gait training is an essential element for independent activities of daily living and performing stair gait training may achieve qualitative improvements in independent and social life activities, and is the most important movement training program among treatment processes for hemiplegic patients who are recovering their lower limb functions. 15 Proprioceptive Neuromuscular Facilitation (PNF) is a method of facilitating the response of neuromuscular mechanism through the stimulation of proprioceptors. The Proprioceptive Neuromuscular Facilitation (PNF) procedures help the patients to gain efficient motor function in stroke. 16 Proprioceptive Neuromuscular Facilitation (PNF) is a method of facilitating the response of neuromuscular mechanism through the stimulation of proprioceptors. The Proprioceptive Neuromuscular Facilitation (PNF) procedures help the patients to gain efficient motor function in stroke. Proprioceptor Neuromuscular Facilitation is an intervention method that standardizes body and limb movements into patterns that can immediately improve stroke patients' gait speed. 17 Proprioceptive senses are important for the treatment and evaluation of patients with damage to their nervous systems, and declines in proprioceptive senses lead to declines in postural control, protective reactions, joint motions, balance ability, and gait ability. 18 Proprioceptive Neuromuscular Facilitation (PNF) is an approach to exercise therapy that uses specific movement patterns in diagonal and spiral directions together with specific techniques that facilitate the increase in strength and muscle function. 19 Proprioceptive neuromuscular facilitation (PNF) treatment is a very effective therapeutic exercise for the improvement of muscle thickness, dynamic balance, and gait, and widely used in clinical settings to improve the physical functioning of stroke patients. 20 A
2. Methods and Procedures
Ethical approval was given. All the participants in the study gave their informed consent after the research purpose and procedures had been explained to them.
3. III.
Participants 30 subjects, male and female post-stroke individuals (mean age 54.00±12.97) were recruited for the study. These individuals all met the inclusion criterion of ability to perform the 6 min walk test, were Brunnstrom recovery stage 2 criteria and MMSE score was more than 23. The presence of musculoskeletal or other cardiovascular problems apart from known and controlled hypertension excluded an individual from the study.
4. IV.
5. Dosage
Bilateral Lower Extremities Proprioceptive Neuromuscular Facilitation patterns.
Each session consisted of D1 and D2 patterns with 10 repetitions x 3 sets of each patterns, which was performed 3 times a week for 4 weeks which is total of 12 sessions.
V.
6. Data Analysis a) Statistical software
The Statistical software namely SPSS 18.0, and R environment ver. 3
7. Result
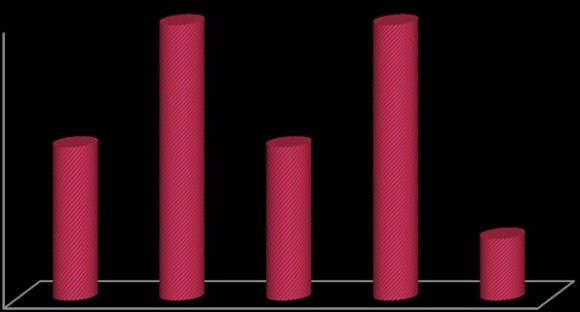
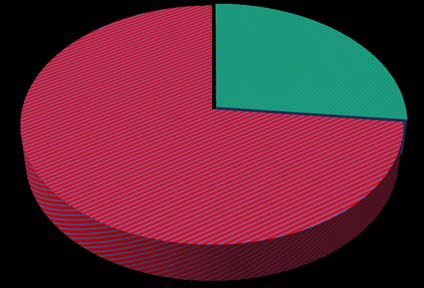
In this study, 30 subjects were recruited, wherein 5 subjects were between the age group of 31-40, which was 16.7% of the entire age category. 9 subjects were between the age group of 41-50, which was 30% of the entire age category. 5 subjects were between the age group of 51-60, which was 16.7% of the entire age category. 9 subjects were between the age group of 61-70, which was 30% of the entire age category and 2 subjects were more than 70 years of age, which was 6.7% of the entire age category. (Table 1, Fig. 1) In this study, among 30 subjects, 8 were female which was 26.7% of the entire gender category and 22 were male, which was 73.3% of the entire gender category. (Table 2; Fig. 2)
8. A
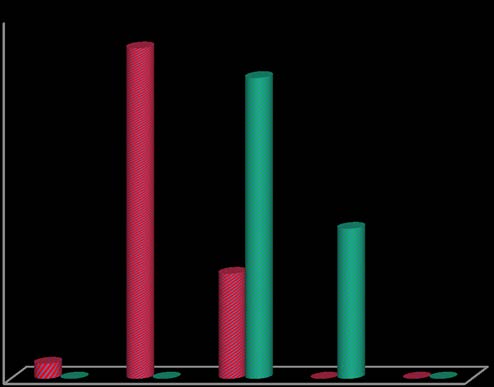
Pre and post test scores of Stroke Impact Scale was evaluated and is shown in Table 3, Fig. 3. In Stroke Impact Scale, there was only 1 subject who scored between 1-20% of the total subject size, which was 3.3% in the pretest score, and no subjects scored between 1-20% in the post test score of Stroke Impact Scale, with the % difference of -3.3%. 22 subjects scored between 21-40% i.e. 73.3% of the total subject size and there was no subject scoring between 21-40% in the post test score of Stroke Impact Scale, with the % difference of -73.3%. 7 subjects scored between 41-60% in the pretest score which was 23.3% of the total subject size and following the intervention, 20 subjects scored between 41-60% in the post test score which was 66.7% of the total subject size, with the % difference of 43.4%. No subjects scored between 61-80% in the pretest score whereas 10 subjects scored between 61-80% in the post test score following the intervention, which was 33.3% of the total subject size, with the % difference of 33.3%. No subjects scored between 81-100% in the pre and post test scores of Stroke Impact Scale.
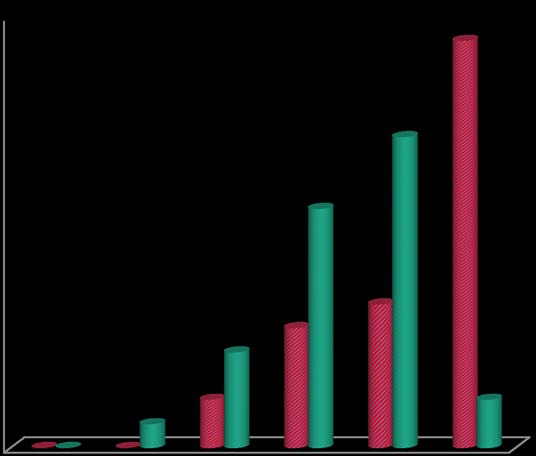
The pre and post test scores were evaluated by applying "paired proportional test", where the p value obtained was P<0.001, which proves that the intervention was statistically significant. 16.7% of the entire subject size and following the intervention, 10 subjects ambulated the stairs within 61-80 secs in the post test score of Timed Up and Down Stairs test, which was 33.3% of the entire subject size, with the % difference of 16.6%. 6 subjects ambulated the stairs within 81-100 secs in the pretest score of Timed Up and Down Stairs test which was 20% of the total subject size and following the intervention, 13 subjects could ambulate the stairs within 81-100 secs in the post test score which was 43.3% of the total subject size, with the % difference of 23.3%. 17 subjects ambulated the stairs within 101-120 sec in the pretest score which was 56.7% of the total subject size and following the intervention, 2 subjects could ambulate the stairs within 101-120 secs in the post test score which was 6.7% of the total subject size, with the % difference of -50.0%. The pre and post test scores were evaluated by applying "paired proportional test", where the p value obtained was P<0.001, which proves that the intervention was statistically significant. Hence, these results depict that all the outcomes had shown significant improvement post intervention.
9. Discussion
A stroke or Cerebrovascular accident (CVA) is defined as an abrupt onset of a neurologic deficit that is attributed to a focal vascular cause.
The purpose of the study was to analyze the effect of lower extremity proprioceptive neuromuscular facilitation patterns on stair ambulation in stroke patients.
Subjects with stroke may experience a variety of deficits, including impairment of motor, sensory, cognitive, perceptual and language functions. They also suffer severe disability to maintain posture and balance within the base of support, which reduces the ability to weight bear on the paretic side during walking and dynamic stability. Stair ambulation is important for independent mobility in Activity of Daily Living. Hence, it is important in stroke rehabilitation to improve the lower extremity activity essential for gait and stair ambulation to increase their Quality of Life (QOL).
Walking is the most basic means of human transport in daily life. Because stair climbing is a common activity of daily living, the ability to do it efficiently is important to an individual's quality of life. More demanding than level walking, stair ambulation is performed with difficulty by the subjects who has decrements in motor function, balance problems, or reduced lower-limb function and rehabilitation population, such as: stroke.
Stair ambulation is one of the most common activity of daily living (ADL). Stroke patients frequently use stairs in their daily life. Stairs are increasingly being used as both an assessment tool and as part of exercise programs. Stairs make an excellent functional assessment measure because they are relevant to people's Activity of Daily Living (ADL)s and have been related to independence and community participation. Of further benefit is the fact that stairs are readily available, convenient, and cheap to use.
Proprioceptive neuromuscular facilitation (PNF) is an intervention method that standardizes body and limb movements into patterns that can immediately improve stroke patients' gait speed and functional ability.
The impact of Lower Extremity Proprioceptive Neuromuscular Facilitation patterns on stair ambulation for stroke patients for the above mentioned disability were analyzed and clinical relevant outcome measures were chosen for the same. Stroke Impact Scale is used to evaluate how stroke has impacted the individual's health and life. Timed Up and Down Stairs test is used to potentially reflect improvements in the musculoskeletal and neuromuscular systems that contribute to the control of posture.
In this study, the intervention is directed on Lower Extremity Proprioceptive Neuromuscular Facilitation Diagonal patterns which involves three components: flexion-extension, abduction-adduction, and internal-external rotation. The pattern activates muscle groups in the lengthened or stretched positions. The patterns are used to improve the patients' mobility and functional ability, which was significantly proved by the statistical analysis.
The intervention is also proven helpful in improving the subjects' Activity of Daily Living (ADL) such as: walking and self-care activities, as well as in housework activities such as shopping and public transport use.
Thus, this study shows that patients after stroke could ambulate the stairs effectively with the help of Lower Extremity Proprioceptive Neuromuscular Facilitation Patterns.
VIII.
10. Limitations
1. The study was carried out on small sample size. 2. No long term follow-up was carried out to assess the carryover effect after 4 weeks of the intervention. 3. The patients who were aged and obese were not much cooperative for the study.
IX.
11. Recommendations
1. Long term follow-up with larger population are warranted to see the effectiveness of the intervention and it might reveal higher statistical significance. 2. Proprioceptive Neuromuscular Facilitation patterns can be used as the functional intervention along with task oriented training.
X.
12. Conclusion
The study conducted was a single group study for a duration of 12 months at Kempegowda Institute of Physiotherapy, Bangalore. The frequency of each session consisted of D1 pattern which was 10 repetitions of 3 sets and D2 pattern which was again 10 repetitions of 3 sets, that was conducted 3 times per week for 4 weeks with the total of 12 sessions. In this study, Proprioceptive Neuromuscular Facilitation D1 and D2 patterns of Lower Extremity is incorporated in the treatment protocol in order to know the effect on stair ambulation in stroke patients.
The impact of Lower Extremity Proprioceptive Neuromuscular Facilitation patterns on stair ambulation for stroke patients were analyzed and clinical relevant outcome measures were chosen.
The outcome measures were used for pre intervention and post intervention assessment with Stroke Impact Scale and Timed Up and Down Stairs test. Accordingly, the subjects were assessed on Day 1 and pretest scores were recorded. Following the intervention, post test scores were recorded after 12 sessions in order to evaluate the effect of Lower Extremity Proprioceptive Neuromuscular Facilitation patterns on stair ambulation.
Following statistical analysis, the comparison within the groups was analyzed using "student t test, i.e. two-tailed, dependent". There was significant improvement in Stroke Impact Scale and Timed Up and Down Stairs test.
Thus, the results observed in this study concluded that, Lower Extremity Proprioceptive Neuromuscular Facilitation patterns was effective in order to improve stair ambulation in stroke patients.
| b) Study design |
| An observational single group clinical |
| assessment study. |
| VI. |
| D D D D ) A |
| ( |
| ? To assess the effectiveness of lower extremity |
| proprioceptive neuromuscular facilitation pattern on |
| stair ambulation in stroke patients, which is |
| analyzed by paired proportion test. |
| © 2019 Global Journals |
| Age in years | No. of patients | % |
| 31-40 | 5 | 16.7 |
| 41-50 | 9 | 30 |
| 51-60 | 5 | 16.7 |
| 61-70 | 9 | 30 |
| >70 | 2 | 6.7 |
| Total | 30 | 100 |
| Mean ± SD: 54.00±12.97 | ||
| Gender | No. of patients | % |
| Female | 8 | 26.7 |
| Male | 22 | 73.3 |
| Total | 30 | 100 |
| Stroke Impact Scale % | Pre Test | Post Test | % difference |
| 1-20 | 1(3.3%) | 0(0%) | -3.3% |
| 21-40 | 22(73.3%) | 0(0%) | -73.3% |
| 41-60 | 7(23.3%) | 20(66.7%) | 43.4% |
| 61-80 | 0(0%) | 10(33.3%) | 33.3% |
| 81-100 | 0(0%) | 0(0%) | 0.0% |
| Total | 30(100%) | 30(100%) | - |
| Timed Up and Down Stairs Test (sec) | Pre Test | Post Test | % difference |
| 1-20 | 0(0%) | 0(0%) | 0.0% |
| 21-40 | 0(0%) | 1(3.3%) | 3.3% |
| 41-60 | 2(6.7%) | 4(13.3%) | 6.6% |
| 61-80 | 5(16.7%) | 10(33.3%) | 16.6% |
| 81-100 | 6(20%) | 13(43.3%) | 23.3% |
| 101-120 | 17(56.7%) | 2(6.7%) | -50.0% |
| Total | 30(100%) | 30(100%) | - |
| P<0.001**, |
| Pre Test | Post Test | difference | t value | P value | |
| Stroke Impact Scale % | 33.64±8.66 | 57.80±6.66 | -24.158 | -16.115 | <0.001** |
| Timed Up and Down Stairs Test (sec) | 96.60±20.73 | 80.50±19.22 | 16.100 | 13.332 | <0.001** |
| Student t test (Two tailed, dependent) | |||||