1. Introduction
alcium apatite deposition disease (CADD) is a common entity characterized by deposition of calcium apatite crystals within and around connective tissues, usually in a periarticular location 1 . Many different locations of CADD have been described amongst which, lateral collateral ligament (LCL) of the knee is a rare location 2 . The first ever case of calcific deposits in the lateral collateral ligament of the knee was reported by Anderson et al 3 in 2003. A few isolated case reports of LCL calcification are published in the literature 4,5 but arthroscopic excision of calcific deposit in LCL has not been described yet in the literature. Here we are describing 2 cases of arthroscopic excision of calcific deposits in LCL of the knee by a new portal called 'Direct lateral portal' for the knee.
2. II.
3. Case Report
Both cases were operated after institutional ethical committee clearance. The 2 cases reported here were operated using the New "Direct Lateral Portal/Bengaluru Chandrashekar Portal" after obtaining written informed consent with a prior explanation of the procedure.
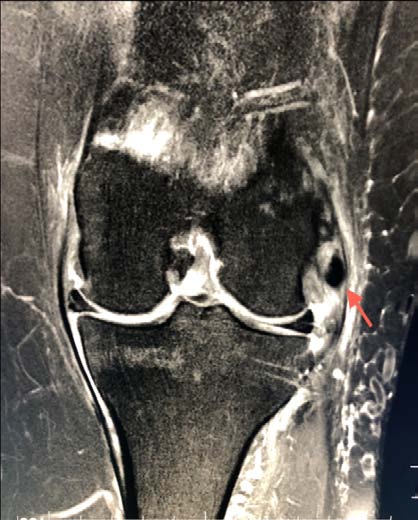
Case 1-A 50-year-old lady presented with pain in the left knee of one year duration. There was no improvement with conservative treatment in the form of anti-inflammatory medication and physiotherapy. X-ray of the knee showed calcification in the LCL region (Fig. 1a 1b). The technique of arthroscopic excision of calcification in LCL.
4. Figure Ia: Calcification in LCL Region
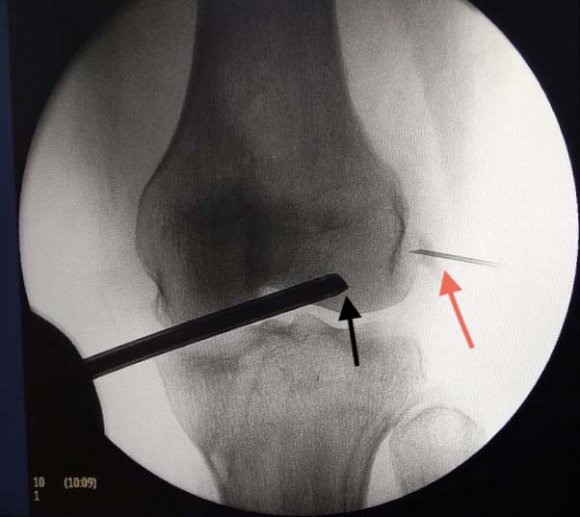
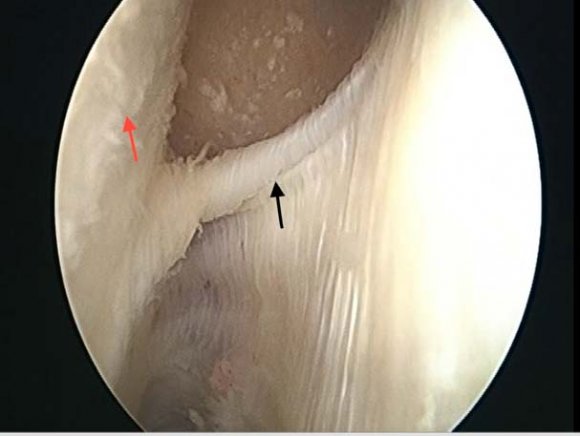
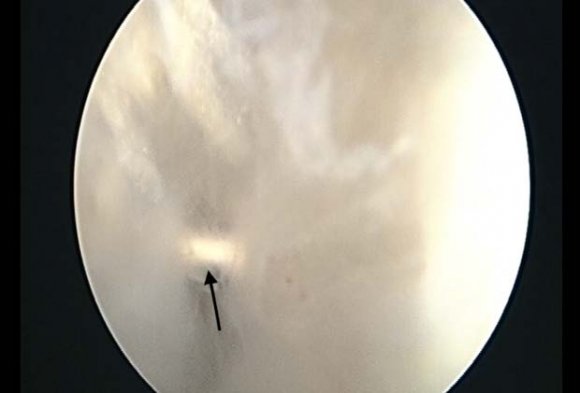
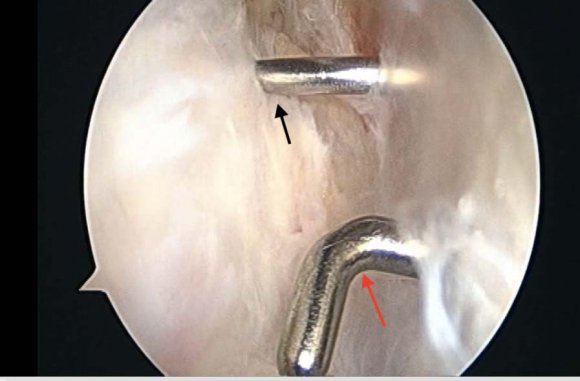
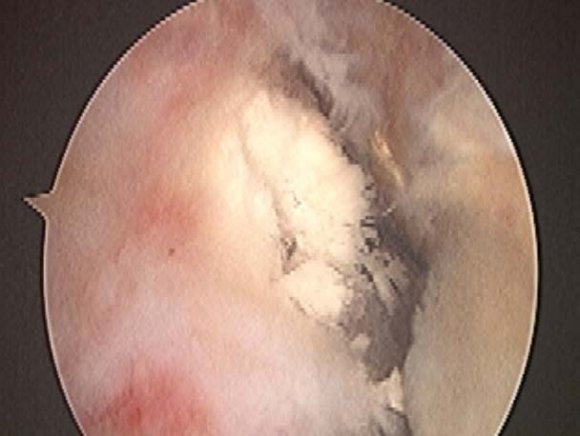
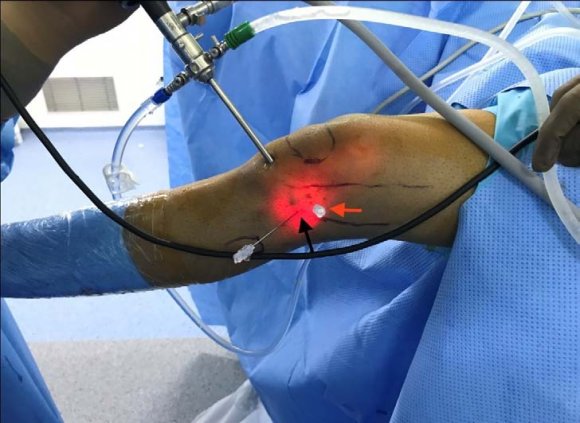
Under spinal anesthesia, the patient is placed in supine position with the limb held by thigh holder, so that the knee is in a hanging down position, making a flexion angle of 90 degrees. Standard anterolateral and anteromedial portals were made. The knee was then positioned into extension with arthroscope in the anterolateral portal. A needle was placed over lateral epicondyle under IITV guidance (Fig. 3). With the arthroscope in the anterolateral portal, the superolateral portal was made. Bands over the lateral gutter (Fig. 4 a) were cleared and then the arthroscope was moved inferiorly and posteriorly until the needle over the lateral epicondyle (Fig. 4 b) was visualized. A direct lateral portal, 1cm inferior and 1cm posterior to the lateral epicondyle with the knee in extension was made (Fig. 4 c and d). The calcific deposits in LCL were visualized (Fig. 4 e). The LCL and popliteus were dissected (Fig. 5), calcific deposits in the LCL was debrided by switching the arthroscope and shaver between the anterolateral portal and direct lateral portals. A small part of the LCL was shaved at the area of calcific deposit and all the deposit was squeezed out. Intactness of the LCL was confirmed with Varus stress test and the opening of the lateral joint was confirmed under IITV guidance (Fig. 6 a, 6b).
5. Discussion
Calcific deposits in the lateral collateral ligament of the knee has been described in the literature [1][2][3][4][5] .The condition is described in the middle and old age group 6 .Open excision of calcific deposit has also been described in the literature 7,8 , but arthroscopic excision has not been described in the literature. In a study by Hyoung Hoo Kim et al 9 , they performed open excision of the calcific deposit which led to the disruption of the ligament, so the ligament had to be repaired back. To prevent ligament injury by the open technique, arthroscopic excision was conceptualized. Our concept of arthroscopic excision for the lateral side of the knee is inspired from a case report by Shenoy PM et al who excised calcium deposit from popliteus 10 .
We considered the feasibility of direct lateral portal and extensively studied and planned the portal. We performed cadaver study on 2 knees at a cadaver lab and further dissected the knee to know the safety of the portal (Fig. 7 a). On cadaver dissection of the direct lateral portal, the skin was incised to reach Iliotibial band (IT) (Fig. 7 b). IT band was excised to visualize lateral epicondyle (Fig. 7c and d Lateral epicondyle is 23.97 mm (sd 3.27) from the distal joint line and 24.42 mm (sd 3.14) from posterior joint line 11 . LCL insertion is located 1.4mm proximal and 3.1mm posterior to the lateral epicondyle in a small bony depression 12 . Popliteus attachment is 18.5mm anterior and inferior to LCL insertion 12 . We safely dissected anterior to the common peroneal nerve and also did not damage the LCL fibers while making the portal.
Looking at the safety of this portal, we performed an arthroscopic debridement of calcific deposit in LCL in 2 patients. Along with standard anterolateral, anteromedial portals, a superolateral portal was made. Through the superolateral portal, bands in the lateral gutter were shaved with arthroscopic shaver and then a 'direct lateral portal' was done 1cm inferior and 1cm posterior to lateral epicondyle to visualize the LCL. This portal is anterior to the anterior border of the fibula, so there is no risk of injury to the common peroneal nerve. Calcific deposits in the LCL were identified and debrided by switching the arthroscope and shaver between the anterolateral portal and direct lateral portals. Finally, intactness of LCL was confirmed by varus stress test and recorded with C-arm. Postoperative X-ray (Fig. 8 a,b) shows the completeness of evacuation of calcification from the lateral side of the knee.
6. Declarations of Interest None
Funding