1. Introduction
he larynx is a winding device of the human body that fabricated voice or speech which are absent in others living being. To generate it, the larynx, particularly vocal cord, should be malleable, organized, and sensible. Phonation is a creation of sound that may be demonstrated by motor activity involves a high orchestration of laryngeal and respiratory neuromuscular regulation. 1 Periaquductal grey matter in the midbrain is an indispensable area for human speech creation. 2 Motor and sensory nerves of the larynx derived from the vagus nerve by way of superior and recurrent laryngeal nerves. The superior laryngeal nerve arises from the inferior ganglion of the vagus and descending to horn of hyoid, where it divided into a small external branches which is only motor supply to the cricothyroid muscle, and a long internal is a sensory supply of larynx above the vocal cord. The recurrent laryngeal nerves in right side leave the vagus nerve by crossing and loops the right subclavian artery and left side crossing the arch of the aorta and running along the inferior thyroid artery in front, behind or between the terminal branches of artery enter into the larynx behind the cricothyroid joint supplies the motor to all muscle of larynx except cricothyroid and sensory below the vocal cord. The superior laryngeal nerve paralysis losses the ability of vocal cord to stretch thyroarytenoid muscle via cricothyroid, consequently recurrent laryngeal nerve unable to tense the other muscle to adduct the cord, therefore it is called adductor paralysis. 3 Due to vocal cord paralysis voice are severely breathy or whispered, hoarseness, reduced loudness and low pitch with possible pitch break. 4 Only recurrent laryngeal nerve lesion where the left side is more than ten times from right side known as abductor paralysis due to contracting, stretching and pulling the-paralyzed vocal cord by cricothyroid muscle towards the midline position consequently the paralyzed abductor muscle are unable to abduct it apart. 5 The most research article showed that most common cause of vocal cord paralysis(VCPS) were iatrogenic. 6 Some reviewers displayed idiopathic was the most common cause of VCPS. 7 Other studies exhibited the common etiological factor was a malignancy. 8 The malignant growth may be created pressure or directly invaded the nerve to generate the VCPS. 9 VCPS is the late symptoms of this diseases of chest, lung, or neck where the surgeon has of the human body which has to execute very associated assignment like protection, respiration, and phonation. To fulfill this mission, the larynx should be accommodated, integrated, and sensible. The vocal cord is the concern of larynx, which served all-purpose. If any occurrence due to iatrogenic, idiopathic, or any other causes shut down the vocal cord mobility, the patient is facing miserable complexity in their life.
Methods: It is a cohort retrospective study of 67 cases in the department of otolaryngology and Head-Neck Surgery, Bangladesh, from 01 July 2016 to 31 June 2019.
Results: Incidence in exchange of prevalence among outpatient was 0.06%, inpatient was 0.37%, and total laryngeal disorder, and thyroid operation was 6.51%. Of them unilateral was 64(95.52%) in which both right and left were equal 32(50%) bilateral were 3(2.99%), male were 28(41.79%), and females were 39(58.21%). Amidst them 00-18 years were 2(2.99%), 19-40 years were 21 (31.34), 41-60 years 36(53.73%) and above 60 years 8(11.94%), smokers were 34(50.74%), betel leaf chewer 26(38.81%), diabetic were 27(40.30%), hypertensive were 19(28.36%), iatrogenic were 33(49.25%), idiopathic 20(29.85%) and others 14(20.90%), 61(91.05%) treated conservatively, 5(7.46%) surgical, and 1(1.49%) denied the repeated surgery.
Conclusion: Hemiparalysis of the vocal cord may produce many inconsistent symptoms, the surgeon may wait for spontaneous recovery, but bilateral paralysis may need immediate surgical intervention to alleviate respiratory obstacles.
2. Keywords: vocal cord paralysis (VCPS), magnetic resonance imaging MRI), computed tomography (CT), rigid laryngoscopy(RL), fiberoptic laryngoscopy(FOL), intraoperative neural-monitoring(IONM).
no option to help the patient except waiting for death. 10 Anaplastic thyroid carcinoma also presented with VCPS. 11 In thyroid surgery, the surgeon facing the VCPS when the patient awaking from the anesthesia or the following day when a patient developing hoarseness, dysphonia, dyspnoea, and aspiration. 12 The surgeon is facing the real obligation when the patient is getting the video of FOL or RL. After complete evaluation by history, examination and investigation like x-ray, CT, and MRI of head, neck, and chest showed nothing abnormalities find out then it declared as unknown etiology which solicited as idiopathic. 13 Brain stroke causes further VCPS in which the Broca's area usually the left frontal lobe in the right-handed dominant person of the Brodmann area 44 and 45 ischemia developing expressive aphasia. 14 Accidental causes of VCPS was few might occurred-due to cut-throat injury or road traffic casualty. 15 About 20% of cases of Guillain-Barre syndrome developed respiratory failure and VCPS and required mechanical ventilation after tracheostomy. 16 In developed countries, they are routinely used IONM in thyroid operation to reduce the VCPS, which wasn't possible in the developing countries due to the high cost of the device. 17 Our aim of the study is to find out the relative incidence and etiological factor of VCPS and pick up the best methods to reduce the calamity of the patient.
3. II.
4. Methods and Materials
It is a cohort retrospective study of 67 cases in the Department of Otolaryngology and Head-Neck Surgery; Cumilla Medical College, Bangladesh from 01 July 2016 to 31 June 2019. During three years period, outdoor patients was 116128, inpatient was 18268, laryngeal disarray patient was 893, and 136 thyroid operation were performed, and these two were total 1029. Hence the Cardiothoracic and Neurosurgery department were sent 11 laryngeal disorder patients who included in 893 patients. We were performed the endoscopic assessment of 1029 patients by rigid Hopkin's laryngeal telescope. The patient and attendant gave the written informed consent about the examination procedure. Of 893, VCPS patient was 34 in which bilateral paralysis were 02; unilateral was 32 whereas the left-sided were 21 and right was 11. Among 136 thyroid operation, VCPS were 33 whichever 1 was bilateral; unilateral paralysis was 32 in that left-sided was 11 and right-sided was 21. Amidst total 67, bilateral was 3; unilateral was 64, astonishing that right and left-sided were equally 32. 66 patients availed the treatment and 01 patients refused the repeated surgery. The following data collected about the patient: Age, sex, personal habit, past illness, and treatment history and postoperative follow up and complication. All data were calculated using the statistical software of SAS.
5. III.
6. Results
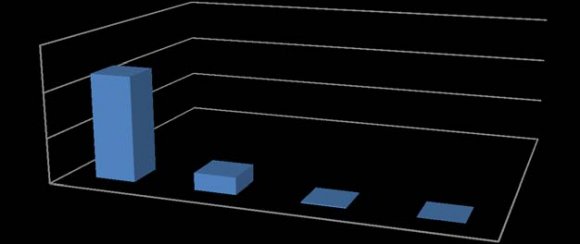
Incidence among outpatient was 0.06%, inpatient was 0.37% and total laryngeal disorder, and thyroid operation was 6.51% (figure-1). From outpatient laryngeal disarray 893 in which VCPS was 34(4.05%), bilateral paralyses was 2(5.88%), unilateral paralyses was 32(94.12%) considering that left-sided was 21(65.63%) and right was 11(34.37%). From inpatient 136 thyroid operation VCPS was 33(24.26%), bilateral was 1(3.03%), unilateral paralysis were 32(96.97%) since left side was 11(34.37%) and right was 21(65.63%) (Figure -2). The average annual incidence was 22.33. Considering from total, 67 bilateral paralyses was 3(4.48%), unilateral was 64(95.52%), whereas surprising that left and right side were equal 32(50% (Figure -3). Among them, female were 39(58.21%), and males were 28(41.79%) (Figure -3). Age allocated 00-18 years were 2(2.99%), 19-40 years were 21(31.34%), 41-60 years was 36(53.73%) and above 60 years were 08(11.94%) whereas lowest one was 17 years, highest was 75 years although mean age was 43.86 years (Figure -4). Personal habits showed smoker was 34(50.74%), nonsmoker was 33(49.26%), betel leaf and nut chewer was 26(38.81%), and nonchewer was 41(61.19%) (Figure -5). Past illness reviled diabetic was 27(40.30%), hypertensive was 19(28.36%), and both combined diabetes, and hypertensive were 13(19.40)(Figure -5). Amidst them iatrogenic was 33(49.25%), idiopathic was 20(29.85%), brain stroke was 06(8.96%), malignancy was 05(7, 46%) in which bronchogenic carcinoma was 04, and esophageal carcinoma was 01, casualty patient was 02(2.99%), and Guillain-Barre syndrome were 01(1.49%) (Figure -6). Treatment option revealed 61(91.05%) were medical, 05(7.46%) were surgical, and bilateral paralysis 01(1.49%) was refused further surgery with a tracheostomy tube in situ. Of surgical 5, 3(60%) were unilateral paralysis given injection augmentation, and 2(40%) bilateral were treated by cordectomy Figure -7).
7. Discussion
There were so many debated about VCPS in the study to study, posibly due to geographical distribution, developed and developing countries with respect to the availability of latest logistic support for surgical procedure. About patient symptoms, all study showed similarly as hoarseness, dysphonia, reduced pitch, pitch instability, respiratory distress, stridor and aspiration. 18 Incidence of VCPS were variable in a different point of view like 0.06%, 0.37%, 4.05%, 6.51% and 24.26% among outpatient, inpatient, laryngeal disarrayed patient, total laryngeal disorder and thyroid operation operative patients and last of all out of thyroid operative patients. The annual incidence was 22.33 where Rathore NS. et al. was 54, which was more than two times of our study whereas Clerf LH. The study showed 23.15 were hold up our observation. 19,20 The relative frequency varies considerably due to causative factors variation. 21 Regarding the side of paralysis, unilateral were more than 95% and bilateral less than 5% in our series, which was carried out by Toutoumchi SJS. et al., study. 22 About the unilateral paralysis right and left both sides were equal, but other studies showed the left side was 02-03 times more than the right side. 23,24 In fact in our study left-sided paralysis were 02 times more than right in laryngeal disarray patient, but in thyroid operation, it was reverse the right side was 02 times more than the left.(Total Thyroidectomy-29, Right hemithyroidectomy-72 and left hemithyroidectomy-35), so both sides were equal out of total VCPS. The reality was that most of our thyroidectomy patient were right-sided and IONM device wasn't used in any operation due to cost. 25 In Government hospital, l 99% of patient are poor and able to expenses a maximum of 50-100 USD for their thyroidectomy, whereas one IONM device is more than 300-800 USD. Concerning gender female was 02 times more than male, which was hold up by Rosenthal et al. series. 26 Since Myssiorek D. et al. series displayed males nearly 02 times more than females. 27 Unclear antecedent was due to in our country, female thyroid operation was seven times more than male. About age in our study, 5 th and 6 th decade showed the highest occurrence, which was reinforced by Gandhi S. et al. series. 28 As regards personal habit and past illness in our study smoker was 34(50.74%), betel leaf and nut chewer was 26(38.81%), diabetic was 27(40.30%) and hypertensive was (28.36%) which was held up by Alassiry H. et al. series. 29 With the reference of our title most common causes were iatrogenic in our study which was thyroidectomy operation was keep up by Ko HC. et al. and Chen HC. et al. series. 30,31 Idiopathic was the second most common cause in our study, whereas Rosenthal LH. et al. series showed it was the third most common cause of VCPS. 26 In our study brain stroke(8.96%) was the third cause of VCPS, which was against the Rubin AD. et al. series. 32 According to UNESCO adult literacy rate of Bangladesh is 72.89%. In our country, one group of people aren't aware of health status, so uncontrolled diabetes, hypertension, unrestrained smoking; betel leaf, and nut chewer were causing brain stroke. Malignancy was the fourth cause in our study, which was also not in our favor whereas Yumoto E. et al. and Rosenthal LH. et al. showed malignancy were the second most common cause of VCPS. 24,26 Casualty was two cases in our study, which was near to Rathor NS. et al. study, they showed, one case. 19 In our study one case of Guillain-Barre syndrome which was supported by Asbury A. K. et al. series. 33 In our study of treatment, 61(91.05%) patients availed medical treatment, 5(7.46%) availed surgery, in which 3(60%) were treated by Inj Calcium Hydroxyapatite for unilateral paralysis, and 2(40%) were treated by cordectomy as sacrificing the voice quality for bilateral VCPS which was reinforced by Jinny Y. et al. and Silva Merea V1. et al. series. 34,35 V.
8. Conclusion
The most common causes of VCPS were iatrogenic, and we are concerned it due to the thyroid surgery was done by the Otolaryngologist. It is a real obligation for us. So before starting the thyroid surgery, every surgeon should be adopted with the surgical anatomy. The latest technology should be provided by the Government for poor people. Before telling the patienst idiopathic, a thorough and unified evaluation should be completed about VCPS patient. Now time is demanding a competent surgeon and latest technical support to reduce the catastrophe of the patient.
![Figure-1: Incidence of VCPS in outpatient, in inpatient and laryngeal disorder+Thyroidectomy patient. [n-116128;VCPS-67(0.06%): inpatient-18268:VCPS-67(0.37%):Larynx+Thyroid-1029:VCPS-67(6.51%)]](https://medicalresearchjournal.org/index.php/GJMR/article/download/2036/version/101292/6-Iatrogenic-and-Idiopathic-Vocal-Cord_html/21403/image-3.png)
![Figure-6: Etiological factor. [n-67; Iatrogenic-33(49.25%):Idiopathic-20(29.85%):Brain stroke-6(8.96%):Malignancy-5(7.46%):Casualty-2(2.99%):Guillain-Barre-1(1.49%)].](https://medicalresearchjournal.org/index.php/GJMR/article/download/2036/version/101292/6-Iatrogenic-and-Idiopathic-Vocal-Cord_html/21404/image-4.png)