1.
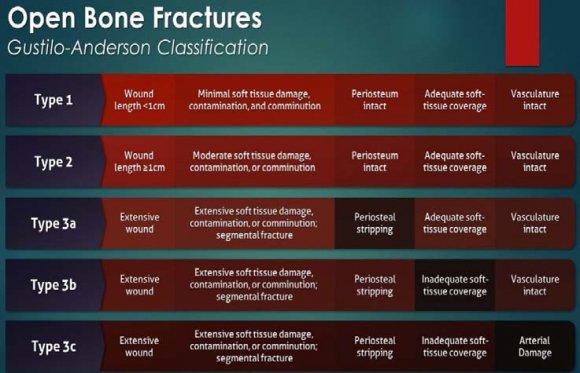
of the femur and tibia when associated with vascular injuries, present major challenges in management. The decision to amputate or salvage can often be a difficult one even for experienced surgeons. Mangled lower extremity results due to high energy trauma especially due to motor vehicle accidents and is defined as injury to three of the four systems in the extremity i.e soft tissues, bone, vascular and nerve. Open fractures are classified by Gustilo and Anderson's classification in which type 3b is a injury where soft tissue loss and primary closure of the wound is not possible and type 3c is any open fracture with vascular compromise.
Case report: We report a case of 27 Years old gentleman who sustained an open 3c Gustilo-Anderson fracture with right floating knee that was initially treated with debridement and external fixator and advised amputation above knee in outside hospital and referred to our hospital for further management.Despite a borderline Mangled Extremity Severity Score (MESS) (Table -2), due to the overall health status of the patient and local clinical status with preserved plantar sensitivity, reconstruction was attempted. After 8 months of treatment, all wounds healed completely with no pain, and satisfactory motor and sensory function was achieved (fig. 18). On examination, anterior tibial artery pulsation was feeble and posterior tibial artery pulsation was absent, subsequently CT right lower limb arteriogram was done after obtaining vascular surgeon opinion. Which reveals posterior tibial vessel under spasm and anterior tibial vessel sluggish blood flow. He underwent right leg and knee wound debridement and reconstruction with ilizarov fixation and soft tissue repair. Subsequently after 7 days he underwent right leg ilizarov realignment and wound debridement with medial gastronemius flap + split thickness skin grafting +vacuum assisted closure (VAC) application (fig. 17). Postoperatively, he was given rehabilitative care and physiotherapy in the form of non weight bearing mobilisation with walker support. The patient was followed up for the period of two years and he is doing symptomatically better.Based on current literature guidelines and evidence-based medicine, management for borderline cases is proposed to aid clinical decision making in these situations.
2. Introduction
angled limb is defined as one that involves a combination of injuries affecting at least 3 out of the four components of the extremity: vascular, nervous, soft tissues and underlying bone. Basically, it is related to type IIIB and IIIC injuries within the Gustilo and Anderson´s classification. However, every work commonly uses criteria that do not always fit within this definition. It is a situation that can lead to amputation in 9% of the cases in the first 24 hours and in 21% during the hospitalization [1].
The term "floating knee" was first described by Blake and McBride in 1975 [2]. It is an ipsilateral fracture of the femur and tibia that includes diaphyseal, metaphyseal, and intraarticular regions of the bone. Floating knee injuries occur as a result of a very highvelocity trauma. Road traffic accidents are the most common cause of this type of complex injuries [3]. The incidence of road traffic accidents are on the rise and are often associated with complex life-threatening conditions and extensive soft tissue damage. Management of these injuries varies according to the type and extent of bony and soft tissue involvement. Bertrand and Andrés-Cano state "although the exact incidence is unknown, this condition is generally rare," the incidence is on the rise currently due to the increased trend in high-velocity traumas. Frequently, multiple produced fractures in the same extremity, will add new dimensions to their management. These fractures range can change from simple diaphyseal to complex articular types.
The degree of severity of open fractures is often classified in accordance with the system of Gustilo and Anderson [5,6]. This takes into account the wound size, fracture pattern and degree of soft-tissue contamination. Type III of this classification corresponds to fractures due to high-energy trauma, with extensive injury to soft tissues, and is divided into three subtypes: types IIIA, IIIB and IIIC, according to the severity of the injury [4,5,6].
The extensive damage seen in types IIIB and IIIC may be a veritable challenge, even for surgeons with greater experience. It may require a clinical decision between attempts to salvage the limb and amputation. Clinical advances within orthopaedic, plastic and vascular surgery have provided the means for reconstructing injuries to limbs that, around 20 years ago, would have resulted primarily in amputation. However, some studies have reported that limb salvage is not always the best solution and that early amputation with prosthetic treatment should be recommended in some cases [7,8].
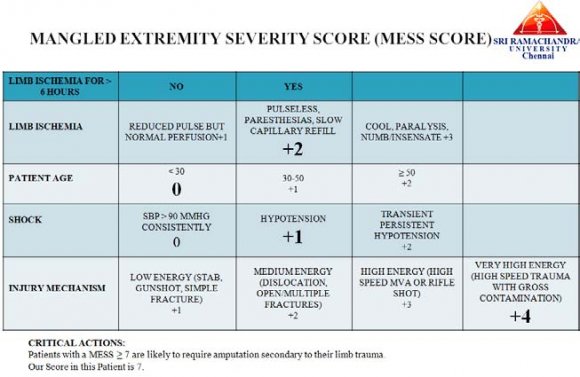
Some classification scores are used to complement the detailed clinical assessment on the affected limb and aid in making clinical decisions [9,10]. Helfet et al. [8] established the use of the Mangled Extremity Severity Score (MESS), which grades injuries based on the clinical findings and takes into consideration the characteristics of the injury, the duration of ischemia, the shock and the patient's age. Scores greater than or equal to seven have predictive value for limb amputation [7].
Although much has been now been reported regarding exposed fractures, there is a gap in the literature in relation to studies presenting a high level of evidence that have compared outcomes between limb salvage and amputation. This gap exists because of ethical concerns regarding randomization of patients between these two procedures [11,12]. Thus, many of the recommendations that are incorporated into the treatment routines for patients with exposed fractures of the tibia and fibula are based on specialists' opinions. Thus, further scientific studies are needed in order to provide scientific backing for surgeons' and patients' choices before the operation.
In the past several decades, limbs with Gustilo type grade IIIC injuries (open fractures of the lower limb associated with vascular injury) have been difficult to salvage and have been treated by primary amputation. With the advancement of surgical technique, especially the use of microsurgery, the salvage rate for grade IIIC lower limb fractures is rising, and the rates of attempted limb salvage are also increasing [13]. Many patients have undergone successful limb salvage [14].These fractures can be managed by reconstruction or amputation. The decision regarding which option to choose can be difficult for both physicians and patients. Complicating this decision is the young age of many of the patients.
In the past, when there were few reliable options for lower limb reconstruction, amputation was the preferred choice because salvage attempts generally used skin grafting, which was inadequate to cover exposed bone [15]. This resulted in high rates of osteomyelitis and secondary amputation [15]. The advancement of microsurgical techniques allowed cooperative efforts between orthopedic and plastic surgeons to reconstruct severe open fractures and achieve predictable limb salvage [16]. Most recently, wound care technology has further increased surgeons' ability to treat open tibial fractures [15].
Reconstruction is performed at a much higher rate than primary amputation, despite the lack of evidence indicating better outcomes associated with reconstruction [15]. It is understandable that both physicians and patients will want to salvage an injured limb. Suffering a serious injury, like an open tibial facture, will have grave physical, emotional and financial consequences, regardless of the treatment method used. The choice of treatment ideally should be based on careful consideration of the available data, however, the overwhelming desire to save the leg, coupled with having the technology to achieve this aim, can cloud the decision-making process for both patients and surgeons.Decision analysis is a powerful tool that can provide evidence when a randomized controlled trial is not practical or ethically feasible. Assigning utilities to these outcomes allows for the comparison and careful examination of complex situations that, otherwise, would be difficult to research.
3. II.
4. Case Report
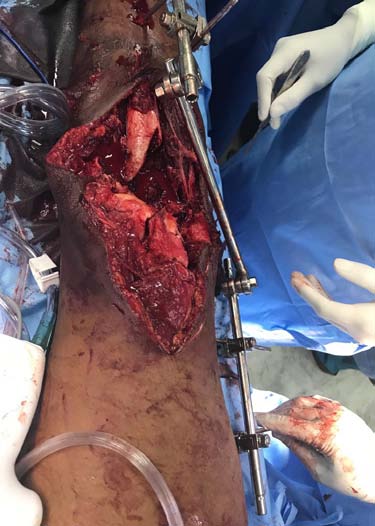
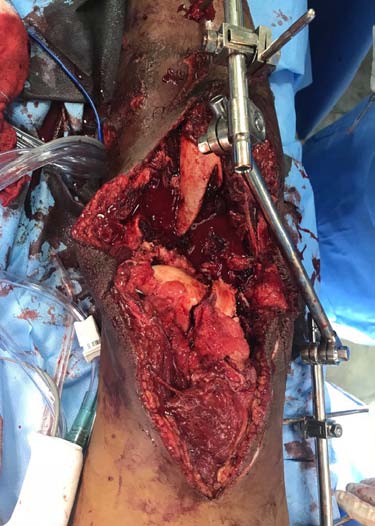
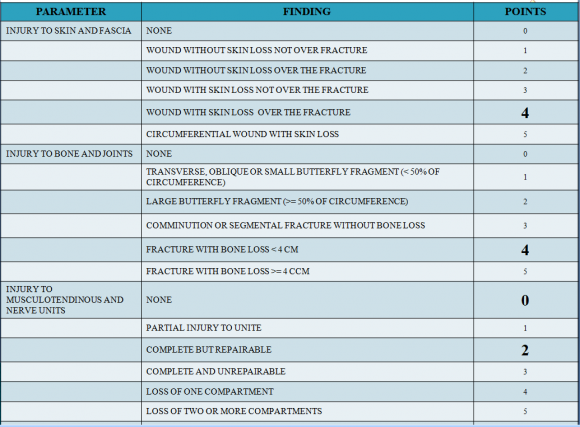
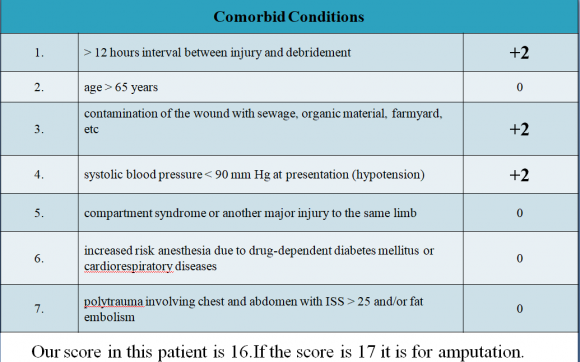
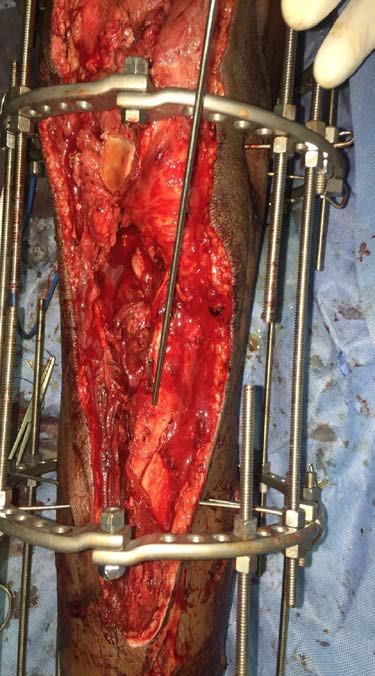
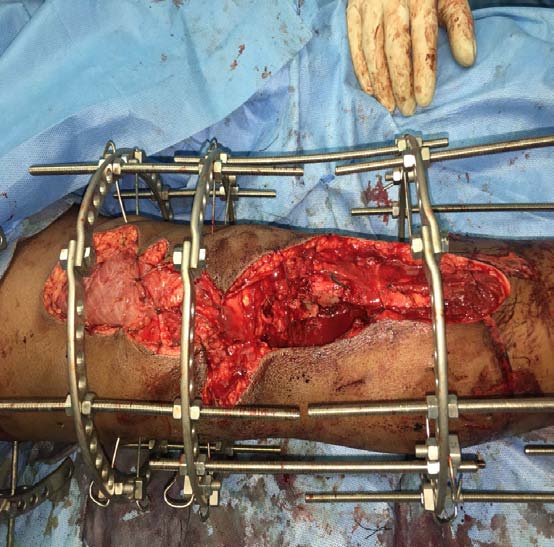
27 Year old gentleman who sustained an open grade 3c Gustilo-Anderson fracture with right floating knee that was initially treated with debridement and external fixator and advised amputation above knee in outside hospital and presented to us within 12 hours of initial injury. On head to toe examination, no other musculoskeletal and organ injuries were present. On initial presentation, he was hypotensive (blood pressure-90/70 mm of hg) and was started on appropriate measures by emergency room team. No known medical co-morbidities were present. He was non smoker, non alcoholic and no drug addiction. On local examination of right lowerlimb: a. Right lower limb knee spanning external fixator present. b. Lacerated wound of size 20x10 cm extending from distal third of thigh to middle third of leg anteriorly. Wound contamination present (fig. 1). c. Both femoral condyle fractured fragments and proximal tibial fractured fragments exposed (fig. 1). d. Patella and lateral tibal condyle absent (fig. 1). e. Tendons and muscles were exposed (fig. 1). f. Dorsalis pedis artery pulsation-feeble. g. Posterior tibial artery pulsation-absent. h. Sensations over right lower limb were intact. -2) was used to assist in the decision of injuries that also had a vascular component and the total score was found to be 7 (? 7 should be consider for amputation). In view of partial vascular injury (Anterior tibial artery pulsation feeble and Posterior tibial artery pulsation were not felt), Ganga Hospital Open Injury Severity Score (GHOISS) was also used which was found to be in borderline range of 16 score (Table -1). Scoring systems provided limited diagnostic benefit. Thus, we had an extensive discussion with the patient and his relatives, in order to point out that any attempt at limb salvage might result to major complications and probably a delayed amputation. In addition, even with salvage severe disability was expected. After discussing and taking consent from patient and his relative he was taken up for combined procedure under orthopaedic and plastic surgery team after obtaining anaesthetic fitness. He underwent right leg and knee wound debridement and reconstruction with ilizarov fixator and soft tissue repair. Intraoperatively, Patella and lateral tibal condyle was found to be absent (fig. 1,5,6). Patella tendon was sutured to quadriceps tendon. Postoperatively, he was shifted to intensive care unit in view of raised serum myoglobin and CPK levels for which cardiology opinion were sought. After 1 week, patient underwent right leg ilizarov realignment and wound debridement with medial gastronemius flap + split skin grafting + vacuum assisted closure (fig. 17). Introperative period was uneventful. Intraoperatively gram, fungal and acid fast bacilli stain and culture was sent and found to be negative for organism growth. Postoperatively regular wound inspection and dressing done which was found to be satisfactory clean (fig. 17, 18). Blood culture and urine culture shows no growth. He was afebrile (initially he was hypotension which was controlled during the course of treatment) and was hemodynamically stable. Gustillo and Anderson´s classification (fig. 4) was used in order to highlight the contamination and the soft tissue injuries as a risk factor in the fracture evolution. It was classified as grade 3c (as vascular injury was present). He was started on rehabilitative care. Range of motion of knee was found to be 0 to 40 degree of flexion with some instability (fig. 18). Strict non weight bearing walking with walker support was encouraged. Quadriceps and hamstring muscle strengthening exercise was started. The treatment was deemed successful and the patient was discharged. Regular xray radiography was taken to assess fracture union (fig. 2, 3, 7, 8-16). Fracture union for distal femur was seen at 8 months and for tibia it was 12 months. He was followed up for the period of two years and he is doing symptomatically better.
5. III.
6. Discussion
Floating Knee Injury (FKI) are uncommon injuries and its true incidence remains unknown. Patients with FKI are usually victims of high speed trauma, mostly motor vehicle accident which involves fracture of femur and tibia. Fracture of two very strong bone of human body required immense force.
It is not just an extremity injury, several organ injuries and multiple fractures are often associated, which can be life threatening. Careful evaluation of patient was carried out to identify other associated injuries and treatment priority should be given to life threatening injury over extremity injury.
The role of early total care (ETC) and orthopedic damage control (DCO) in polytrauma has always been a controversial issue. In stable patients, ETC is more appropriate and in unstable patients DCO is required. However, considerable doubt remains in borderline patients. Some author advised ETC in all patients except in more critical patients and some advised DCO and delayed skeleton stabilization [17].The literature has also reports utility of serum lactate to assess timing of treatment and mortality, but its role is still controversial to predict survival after major injury [18]. In our case report, we did not measure serum lactate level.
The incidence of amputation was reported to 27% in FKI which had massive soft tissue crushing, severe infection and neurovascular injuries [19].
Blake and McBride [20] defined the floating knee injury as the ipsilateral fractures of the femur and the tibia. Fraser et al. in year 1978 classified floating knee in more detail [21]. This classification was again modified by Letts and Vincent [22] in 1986 which included soft tissue injury associated with these injuries.
Decisions making in clinical situation of Mangled Extremity in complex as number of factors are involved [25]. These factors are: Patients who initially confront a threatening injury often focus on the loss of the extremity rather than on the consequences of the limb salvage. Patients undergoing this procedure, will require more complex operations, longer hospitalization, and will suffer more complications than primary amputees. Tornetta and Olson reported on patients who have undergone multiple operations over a period of several years to "heroically" save a leg only to render the patient depressed, divorced, unemployed, and significantly disabled [23]. Unfortunately, "salvage" of a mangled extremity is no guarantee of functionality or employability. It is crucial for the patient and his family to realize that both salvage and early amputation by no means can reassure the patient that will return to a previous normal, pain free extremity [24]. In our case report, patient is doing well after limb salvage surgery. Functional improvement has been seen during the follow up periods (fig. 18).
Significant indicators of poor outcome results of floating knee injuries are intra-articular involvement of the fractures, severity of skeletal injury, and severity of soft tissue injuries. In most of the patients, sepsis and other infection complications may be so severe and persistent that ultimately secondary amputation is required. Bondurant et al. [26] compared primary versus delayed amputations in 43 cases, including 14 primary and 29 delayed ones. Important findings included 6 deaths from sepsis in delayed amputation group compared with none in the early amputation group. In our case report, no clinical and laboratory evidence of sepsis were noted.
Although cost should not be a major deciding factor for limb salvage, many patients may be devastated by the cost, not only of medical bills but also of time off work [26]. Fainhurst [27] retrospectively compared the functional outcome of patients who sustained traumatic below knee amputations with that in patients who underwent limb salvage of Gustilo type III open tibial fractures. All patients in the early amputation group returned to work within 6 months of injury, while those who underwent late amputation and salvage returned to work an average of 36 and 18 months after injury, respectively. The authors recommend an early amputation when confronted with borderline salvageable tibial injury. In our case report, patient returned to his work after 12 months following injury.
Fagelman et al. [28] evaluated the correlation between fractures of Gustilo and Anderson types IIIB and IIIC and the MESS index for exposed fractures of the lower limbs and found results that significantly predicted treatment, for 93%. On the other hand, Sheean et al. [29] did not find any significant difference in MESS values between amputees and patients whose limbs were salvaged. Both of these authors highlighted the importance of the presence of vascular lesions as a factor predictive of amputation. Slauterbeck et al. [30] reported that early use of a scoring system such as MESS would possibly reduce the morbidity associated with prolonged hospital stay and with the various surgical procedures performed in these cases.
The most widely described scoring systems are: the Mangled Extremity Syndrome Index (MESI) [31], the Predictive Salvage index (PSI) [32], the Mangled Extremity Severity Score (MESS) [9], and the Nerve Injury, Ischemia, Soft-Tissue Injury, Skeletal Injury, Shock, and Age of Patient (NISSSA) Score [11]. Each scoring system has a "cutoff point". If the total score exceeds the critical "cutoff point" primary or early amputation should be considered. However, these scoring systems have been criticized as being too complex and subjective with large variations in interobserver classification of mangled extremity, and as expected none of them is accurate in all cases [33]. Even among experienced surgeons there is disagreement regarding the criteria of these scoring systems, which cannot be used with confidence in clinical practice, because their use has not led to specific outcomes.
In our case report, inspite of MESS score (Table -2) of 7 which is suggestive of amputation, we have chosen the option of salvaging the limb after considering the patient factor. With MESS score of 7 or greater, amputation is the eventual result. No scoring system, however, can replace experience and good clinical judgment. It needs to be remembered that advances made in limb salvage surgery has been matched by advances in amputation surgery and prosthesis design. More often, however, the choice between limb salvage and amputation must be made on the basis of expectations and desires of individual patient and the family.
Although scoring systems may be helpful, the patient's status cannot simply be summarized by a score number. A closer look reveals that many questions remain unanswered. These systems fail to consider factors related to the patient's quality of life, pain, occupation, age, wishes, social support system, family status, and financial resources. The training and experience of the surgical team may also influence the decision to amputate or reconstruct. Although these considerations are more subjective, undoubtedly they are very important. The true measure of successful limb salvage lies in the overall function and satisfaction of the patient. In our case report, the main reason for limb salvage, despite the indication for amputation according to MESS and borderline ganga scoring system (score of 16) (Table-1), it was patient and physician's choice in relation to his occupation, condition and psychology.
The final decision regarding the treatment for patients with a diagnosis of an exposed fracture of the tibia needs to take into account future functionality, availability of recovery, the patient's profile and the surgeon's expertise. The criteria for indicators such as the MESS score and the fracture classification need to be carefully analyzed so that the limb salvage can be done in an effective manner and so that amputation is done in precisely selected cases.
There are many studies in literature suggesting internal fixation of both the fractures of floating knee should be done as early as possible [35]. Ratliff found that internal fixation of both fractures was less likely to cause the development of knee stiffness and lessen the duration of hospital stay [36]. Ostrum treated patients with retrograde femoral nailing and antegrade tibia nailing through 4 cm medial parapatellar incision [37]. The average time to union of femoral fracture was 14.7 weeks and for tibial fracture was 23 weeks. Theodoratos et al. [21] recommended intramedullary nailing as the best choice of treatment, except for grades IIIB and IIIC open fractures. In our case report, patient was treated with initially by application of external fixator followed by ilizarov fixator application. Time to union of femoral fracture was 8 months and for tibia fracture was 12 months.
In literature we found that outcome of FKI were often variable, some author reported 0 excellent result and other author reported excellent result up to 53%. These variable results might be due to associated neurovascular injury, open fracture and variable fracture pattern with FKI [34] Severe trauma to the lower extremity with vascular compromise often leaves the surgeon with a very difficult clinical decision; whether to salvage or amputate [39,41,46]. With today's therapeutic and technological advances, the trauma surgeon has the ability to salvage viability in most, if not all, severe lowerextremity injuries. Obviously, there have been some remarkable successes and, unfortunately, some horrendous failures. Patients have suffered protracted hospital courses, multiple surgeries, multiple subsequent hospitalizations, complications (especially infections and nonunions), and the inevitable delayed amputation of a viable but nonfunctional extremity [39,43,46]. The major decision in open fractures of the lower extremities with vascular compromise is not whether one can but whether one should attempt salvage. This decision is often clearly mandated by the nature and extent of the lower-extremity injury and the patient as a whole. Lower-extremity replantation, except maybe in children, is clearly unwarranted. Lang et al. have shown that division of the posterior tibial nerve as part of the lower-extremity injury in adults is an absolute indication for amputation [42]. Recent literature supports the overall poor prognosis for successful salvage for Type IIIC tibial injuries (open tibial fractures with vascular insufficiency) [6,38,42]. The occurrence of a crush injury and/or warm ischemia longer than six hours makes limb salvage futile. The traumatized patient with vascularly compromised open fractures in the lower extremity requires prioritization of life-saving procedures and is often best served by amputation. However, there are a large number of patients with lower-extremity injuries with vascular compromise who do not fit the above criteria for primary amputation. Recent literature has stressed the need for establishing objective criteria to assist the surgeon in the urgent decision for salvage versus primary amputation [39,41,46].
Even though the predicted value for amputation of a MESS score higher than or equal to 7 appears to be very high, with larger numbers there inevitably will be a limb with a score of higher than or equal to 7 that will be salvaged, or a limb with a score of lower than or equal to 6 that will require delayed amputation.
7. IV.
8. Conclusion
As a majority of cases represent a "gray zone" of unpredictable prognosis, and borderline cases are a dilemma, the decision to amputate or not amputate should not always be made during the initial evaluation. Although scoring systems and "cutoff points" are useful, the final decision for limb salvage should be based on team experience, technical skills, multidisciplinary consultation, tertiary-care facility, and the profile of the patient. Scoring systems should be used only as guides to supplement the surgeon's clinical judgment and experience. Excellent clinical and functional outcomes can be achieved with individualized planning of treatment which is dependent on the patient's general condition, type of fracture, and severity of soft tissue injury by an experienced multidisciplinary team instead of a fixed definite management for all patients.
With great effort and good team work (like vascular and orthopaedic surgeons) badly comminuted compound injuries (Type III C injury) can be managed well with Ilizarov fixation. Even though the decision of amputation versus Salvage was based on more scientific / scoring system, patient's option should be taken, especially in borderline cases considering the present medico legal scenario.