1. Introduction
troke is a common neurological disorder, the second commonest overall cause of death, and a major cause of disability in survivors. 1,2 Cerebrovascular disease is globally the sixth commonest cause of an ongoing disease burden, but is expected to move to the fourth place by 2020,Over65% of stroke deaths are reported from developing countries. 3,4 Stroke is largely preventable, so that knowledge of risk factors is essential to achieve a reduction in the stroke rate and resulting diseaseburden. 5 Examination of stroke incidence, prevalence, subtypes, risk factors and outcome in various countries is therefore an important foundation for evidence-based prevention programs. 5 Although epidemiologic studies on stroke were carried out in different parts of the world including some neighboring Arab countries, there were no published data from Egypt. 5 II.
2. Subjects and Methods
A total of 504 patients, admitted to A in Shams University Specialized Hospital stroke unit during the period from January 2011 to March 2012 with a diagnosis of acute cerebral stroke, were subjected to the following:
? Detailed medical history taking. Table (3) shows that the mean NIHSS on admission was (7.97±4.91) with median score (7), while the mean NIHSS on discharge was (4.87±3.47) with median score (4). The mean MRS on admission was (3.16±1.33) with median score (3), while the mean MRS on 3 months follow up was (1.87±1.38) with median score (1). Table (4) shows that subtype of acute ischemic stroke among 447 patients of study cases were classified according to "TOAST" criteria into (Figure 1): Table (5) shows that (35.4%) of the study cases showed patent IC large vessels by TOF MRA. (27.4%) of study cases showed IC large vessel with <50% stenosis. (22.9%) of study cases showed IC large vessel with >50% stenosis. And (14.3%) of cases showed totally occluded IC large vessel (Figure 2).
3. Discussion
Although epidemiologic studies on stroke were carried out in different parts of the world including some neighboring Arab countries, there were no published data from Egypt. 5 This study revealed that the mean age of study cases was (63±10.9 years). Males represented (67.1%) of study cases. our results were close to thirty one articles reviewed from different Arab countries. 5 All studies except two found stroke more commonly in males than females (range for males 55.9-75%). 5 One study from Saudi Arabia showed an equal ratio of males to females and another from Kuwait showed a slightly higher female preponderance at 51.7%. 9 The incidence of stroke, as expected, increased with age. 5 This study revealed that (95%) of the study cases were ischemic strokes, while (5%) of study cases were hemorrhagic strokes (all were intracerebral hemorrhage). Our results showed higher incidence of ischemic strokes in comparison to Arab countries, in which ischemic stroke was the commonest type in all series, ranging from 55-87%, while cerebral hemorrhage occurred in 6.3-41. 3% and subarachnoid hemorrhage in 1-9%. 5 This study revealed that subtypes of acute ischemic stroke among cases were classified according to "TOAST" criteria into: Small vessel disease (lacunar strokes) (54.4%), Large artery atherosclerosis (32.0%), Cardio embolic strokes (4.0%), strokes of undetermined etiology (8.9%) and strokes of other determined etiology i.e. vasculitis due to collagen disease (0.7%). Regarding Arab countries, Non-lacunar infarction represented 33-65.5% of strokes while lacunar infarction was reported in 10-35% of patients. 5 these results emphasize our finding of the higher preponderance of lacunar infarction among current study cases (54.4%).
This study revealed that the most prevalent risk factor for stroke among cases was HTN (70.1%), followed by DM (53%), and Heart diseases (35.4%) with "ISHD representing (22%), AF (5.9%), and MI (1.4%), PH of stroke was present among (30.4%) of study cases. Smoking (25.7%).
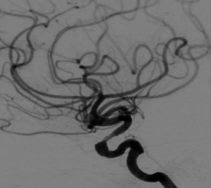
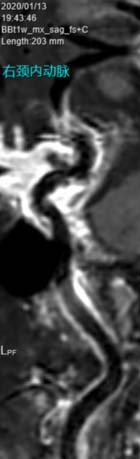
Hyperlipidemia was present among (8.9%) of study cases, while PH of TIAs was found among (8.7%) of study cases, PH of cerebral hemorrhage among (2.4%) of cases, and alcohol consumption (0.4%). Regarding Arab countries, HTN was the most frequent risk factor among stroke patients, being present in 24.9-76% of reported patients, followed by DM which was present in 11.6-69.4%. Hyperlipidemia was reported in 4-61% of patients. And other risk factors were as follows: cardiac disease 5-50%, cigarette smoking 1.6-44%, and previous transient ischemic attack 2.1-46%. 5 these results came in concomitant with our findings of the higher prevalence of HTN and DM. This study revealed that (35.4%) of the study cases showed patent IC large vessels by TOF MRA collapsed image, while (64.6%) of the study cases showed stenotic and occluded IC large vessels as follows: (27.4%) of study cases showed IC large vessel with <50% stenosis, while (22.9%) of study cases showed IC large vessel with >50% stenosis. And (14.3%) of cases showed totally occluded IC large vessel.
These results emphasized findings of previous many studies in populations of Asian, African, and Hispanic descent that demonstrate the preponderance of intracranial stenosis compared with extra cranial carotid stenosis. 10 In contrary to the developed world, in which imaging research has largely focused on extra cranial atherosclerosis, with lower incidence of intracranial stenosis in its white population. 11 Asubstantial study of 300 stroke fatalities in Paris showed that intracranial atherosclerotic plaque occurred in 59% of patients and 37.2% of all patients had intracranial plaque that was stenotic. 10,12 V.
4. Conclusion
Ischemic stroke is the most prevalent type of stroke (95%), Lacunar stroke (54.4%) is the most prevalent ischemic stroke subtype, HTN (70.1%)is the most prevalent risk factor for stroke. IC large vessel stenosis was prevalent among (64.6%) of study cases.
5. VI.
6. Recommendations
Effective primary and secondary prevention of stroke would not be possible without a thorough understanding of the relevant risk factors and stroke subtype.MRA Brain is an important investigative tool for detection and estimation of intracranial (IC) large vessel stenosis which represents a challenging and important clinical situation in everyday neurology practice especially among stroke specialists.


| ? Complete neurological examination with NIHSS |
| score and m RS score. |
| ? CT brain without contrast for all study patients within |
| 30 minutes of clinical suspicion of a stroke at the |
| emergency room(ER) to differentiate acute cerebral |
| infraction from anacute cerebral hemorrhage. |
| ? MRI brain Stroke protocol for 456 patients of the |
| study group within 24 hours of patient admission to |
| the hospital. This protocolin cluded T1-weighted |
| image (T1WI), T2-weighted image (T2WI), fluid- |
| attenuated inversion recovery (FLAIR) image, |
| diffusion weighted image (DWI), gradient-echo (T2*) |
| weighted image MRI scans in addition to TOF MRA. |
| ? Noncontrast 3 Dimensional time of flight (TOF) MRA |
| for anterior and posterior circulation with "collapsed |
| image" films were read and evaluated by |
| Neurology-Radiology team for consensus and |
| agreement of our independent observation of the |
| presence of intracranial (IC) large vessel arterial |
| stenosis or occlusion in (2 Internal Carotid Arteries |
| ICAs, 2 Middle Cerebral Arteries MCAs, Basilar |
| artery BA, 2 Posterior Cerebral Arteries PCAs) |
| among 314 patients of the study group. |
| ? TOF MRA Stenotic lesions are sites where flow signal |
| intensity loss commonly occurs. Stenosis was visually |
| N | % |
| N | Mean | ±SD | Minimum | Maximum | Median | |
| NIHSS on admission | 476 | 7.97 | 4.91 | 1.00 | 27.00 | 7.00 |
| NIHSS on discharge | 391 | 4.87 | 3.47 | .00 | 18.00 | 4.00 |
| MRS on admission | 465 | 3.16 | 1.33 | .00 | 5.00 | 3.00 |
| MRS on 3 months | 340 | 1.87 | 1.38 | .00 | 5.00 | 1.00 |
| study cases | |
| N | % |
| N | % |