1. Introduction
n 31 st Dec 2019, Wuhan Municipal Commission, China, reported a cluster of 27 pneumonia cases of unknown etiology. [1] Samples tested positive for novel coronavirus.
On 30 th January, 2020, WHO declared this outbreak of novel coronavirus as "A Public Health Emergency of International Concern" [2,3]. A large number of cases have been diagnosed Globally. On 11th March 2020-WHO declared COVID-19 as a Global Pandemic. [4] Author ? ?: Department of obstetrics and gynecology, Grant Govt Medical College, Mumbai, India. e-mail: [email protected] Despite extensive studies on the epidemiology of COVID-19 infection, studies on pregnant women with COVID-19 diseases remain relatively less. The physiological changes occurring during pregnancy make pregnant women more vulnerable to corona infection.
The purpose of this study is to summarize the maternal and fetal outcome in COVID-19 pregnancies.
2. II.
3. Material and Methods
An observational study conducted over two months (June2020-July2020) in the Department of Obstetrics and Gynaecology, at a COVID care center, Cama and Albless Hospital, Mumbai, India. A total of 192 women tested positive for COVID-19 by RT-PCR method either antenatally or postnatally are included in this study.
4. Inclusion Criteria
? COVID positive women beyond 28 weeks of gestation. ? Women tested positive for the corona virus within five days of delivery.
Exclusion Criteria ? Women who were less than 37 weeks of gestation. ? COVID negative pregnancies. ? Women tested COVID positive after five days of delivery.
III.
5. Results
The study included a total of 192 women with COVID positive status diagnosed by the RT-PCR method, and we noted the following observations.
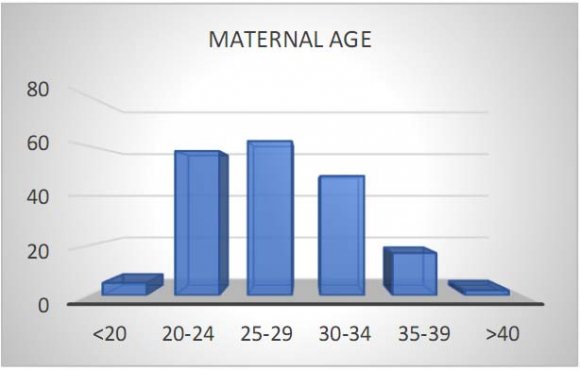
6. Maternal age affected with COVID-19
Majority of the COVID positive pregnant women belonged to the age group of 25-29yrs(32%), followed by 20-24yrs(30%), 30-34yrs(25%), 35-39yrs(9%), 3% are less than 20yrs and 1% are above the age 40years.
7. Parity of the patient
As per the observation made, COVID-19 is more prevalent in primigravida 35%, followed by gravida two 27%, 23% is gravida three, 7%, and 8% are in seen in gravida four and five respectively.
8. Symptoms of patients
In our study, fever (65%) was the most common symptom, followed by shortness of breath(60%), cough(25%), cold and anosmia (15%), loss of taste sensation(10%) vomiting(10%), diarrhea(5%) and generalized weakness(5%).
9. Comorbidities
In this study, 37% of COVID positive patients had Preeclampsia, thyroid disorders were found in 28% women, 21% were anemic, 9% of patients had a past history of tuberculosis, 5% had gestational diabetes.
10. Period of gestation
According to the study done in our hospital, 74% of pregnancies extended till term, and 26% delivered before 37 weeks of gestation.
11. Outcome
In our study, out of 192 patients, 116(60%) delivered vaginally, 55(29%) underwent cesarian section, and 21(11%) patients were discharged with follow-up advice.
12. Discussion
In our study, the Majority of the COVID positive pregnant women belonged to the age group of 25-29yrs(32%), followed by 20-24yrs(30%), 30-34yrs(25%). While a study conducted by MJ Blist and coworkers [5] showed 6(46%) out of 13 patients were of >35years of age.
As per the observation, COVID-19 is more prevalent in primigravida 35%, followed by gravida two 27%.
In our study, fever (65%) was the most common symptom, followed by shortness of breath(60%), cough(25%), cold(10%), vomiting(10%), diarrhea(5%) and generalized weakness(5%).Similarly, in a study done by Paudel SS et al., fever was the most common symptom(17%). [6] In this study, 37% of COVID positive patients had preeclampsia, 28% had thyroid disorders, 21% were anemic, 9% of patients had a past history of tuberculosis, 5% had gestational diabetes. Similar results were found in a study conducted by MJ Blist and coworkers, 23% had pregnancy-induced hypertension, 15% had a past history of lung disease, 8% had gestational diabetes. [5] According to the study done in our hospital, 74% of pregnancies extended to term. 26% delivered before term gestation while in a study conducted by Mullins and colleagues, [7] 47% of the COVID positive women delivered before 37 weeks of gestation.
In our study, the majority of the patients delivered vaginally (60%), and the cesarian section rate was 29%, unlike the research conducted at BMJ where the cesarian section rate was 59%. [8] In our institution, 10% of the patients required intensive care unit admission, seven patients required mechanical ventilator support, whereas in a study conducted by Vinayak Smith, Densearn Seo et al, 30% of the patients required ICU admission. [9] As per this study, there were 4%(7 out of 192 patients) maternal death among COVID positive pregnant women at our institution. There was complication in 8 out of 20 ICU admitted patients with pneumonia, and six patients had acute respiratory distress syndrome, and two patients had septicemia. Three among seven patients were pre-eclamptic, and two patients had a previous history of Koch's etiology. Per se only two maternal death has occurred in the patients without having any pre-existing medical conditions, which accounts for 1% of the maternal death rate.
While in a study carried out by Forestieri, Migliore, et al., two out of seven (28%) women died who were tested positive for the Corona virus. In our institution, among 171 babies born to COVID positive women, we noted that a higher percentage (77%) of babies weighed more than 2500gms. 23% of babies had weight less than 2500gms.
According to this study, 38% of the babies born to COVID mothers required NICU admission for various reasons; fetal respiratory distress being the most common cause. Similarly, in a study conducted by Yan-Ting Wu, et al. Of 30 neonates, 18 (60%) required NICU admission, 12 of hospitalized neonates presented with features of pneumonia. [11] As per the observation made, the majority of the babies born to COVID positive mothers tested negative (87%), and 13% tested positive for coronavirus. Similar results were found in a study done by Rui, Wang, and coworkers [12], where only 2% of babies tested positive among 493 infants tested for SARS-COV-2.
In our institution, we observed only one (5%) neonatal death among 21 babies who tested positive for the Corona virus. The cause of death was type 1 respiratory failure with thick meconium aspiration syndrome with persistent pulmonary hypertension with septic shock, 95% of COVID positive babies recovered successfully.
V.
13. Conclusion
In our study, we observed that the COVID-19 could cause mild-lethal disease in pregnant women and neonates. Most of the women are asymptomatic or have a mild illness, but some of them require intensive care. Pregnancy represents highly adaptive immunity, allowing pregnant women to become tolerant of her fetus yet remain immunocompetent. So per se, pregnancy and childbirth do not increase the risk of acquiring SARS-COV-2 infection. However, pregnancy with high-risk factors like age >35years, pre-eclampsia, preexisting lung pathology, diabetes, obesity increases the inflammatory response (cytokine storm) and may worsen the clinical course of COVID-19. Health care providers should be aware of the epidemiology of Coronavirus disease. The evidence of Vertical transmission appears equivocal. There is no evidence to suggest contraindication to vaginal delivery. Use of proper precautionary measures like regular ANC checkups, use of mask, sanitization, maintaining social distance, educating the community regarding the same, early diagnosis, cater to the required investigations, close follow up, isolation, or in-patient admission if required reduces the maternal and fetal morbidity and mortality.
Modular infrastructure, facilities offered at Tertiary Care Centre such as well-equipped operation theatre, NICU, ventilator availability, NST monitoring, monitoring of feto-maternal wellbeing, expert obstetrician, neonatologist, anesthesiologist, medicine team plays a critical role in safe delivery and good health of both mother and neonate.