1.
Fatine El Alami ? , Rayad Rachid ? , Imane Adnane ? , Salma Chikhaoui ? , Adil Mchachi ¥ , Laila Benhmidoune § , Abderrahim Chakib ? & Mohamed Elbelhadji ? Abstract-Myopia affects approximately 25% of the population.
High myopia is defined by a refractive error of more than -6D or an axial length of more than 26 mm (1-3), it is accompanied by degenerative changes in the eye tissues. It is recognized as a risk factor for the onset of cataracts. (4) Our present work aims to assess the difficulties, peculiarities, and complications of cataract surgery in highly myopic eyes.
Materials and methods: We conducted a prospective comparative study, were included 79 highly myopic patients scheduled for cataract surgery (LA> 26 mm) and 80 patients candidates for cataract surgery as a control group. Patients with pseudo-exfoliation, glaucomatous syndrome, operated for retinal detachment, or with a history of uveitis were excluded. Statistical analysis was performed by SPSS software.
Results: The mean age was 59 ± 9.26 years in the case group and 69.82 ± 10.47 in the control group and for the control group. For highly myopic eyes, the mean axial length was 28.35 ± 1.77 and the mean power of IOL 6.27 ± 6.26. Nuclear cataract was more common in the case group compared to the control group. The duration of the procedure as well as the peroperative complications were comparable between the two groups. After an average follow-up period of 15,8 months, 32% of highly myopic patients required using the YAG laser for secondary cataract, 3 cases of retinal detachment were identified in the highly myopic group, and only one case in the control group.
Discussion: High myopia is a risk factor for the occurrence of cataracts. Its early onset has been confirmed by numerous studies. Cataract surgery in highly myopic eyes can be difficult for various reasons including the implant calculation which can be imprecise, the higher risk of complications during retro and peribulbar anesthesia, zonular fragility as well as the increase of the depth of the anterior chamber. Postoperatively, high myopic people have a higher risk of retinal detachment.
2. Conclusion: Despite the modern techniques and technologies
of cataract surgery, high myopia represents a challenge for surgeons at the different stages of treatment. It is essential to take pre-and intraoperative precautions, as well as postoperative monitoring.
3. Introduction
igh myopia is defined by a refractive error of more than -6D or an axial length of more than 26 mm. it affects about 2% of the population (5), it is accompanied by degenerative changes in eye tissue. It's also a risk factor for cataract formation. Cataract surgery in highly myopic eyes is a technical and refractory challenge for the surgeon (6), it's characterized by the precocity of its onset, the difficulties of its perioperative management, as well as the high risk of retinal detachment.
The aim of our study is to analyze the epidemiological and clinical profile and to assess the different peculiarities in the surgical management of cataracts in highly myopic eyes; as well as postoperative complications.
4. II.
5. Materials and Methods
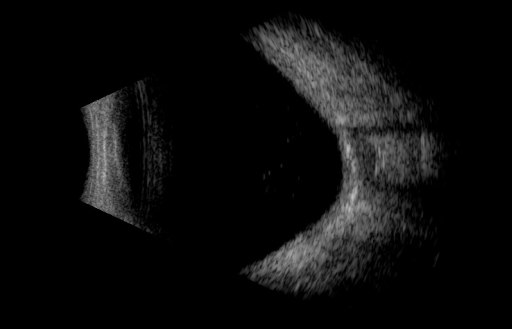
We conducted a prospective comparative study in our department, Were included in this study: 159 candidates for cataract surgery: 79 patients with high myopia (HM) with LA> 26mm (We chose axial length as the parameter because a nuclear cataract with a normal axial length and a normal keratometric value can result in refractive myopia), and 80 non-high myopic (non-HM) patients as a control group. We excluded patients with pseudo-exfoliative syndrome, followed for degenerative vitreoretinal pathologies or with a history of posterior segment surgery, eye trauma or uveitis. When both eyes of a patient were involved, one eye was selected randomly. all patients underwent a complete ophthalmologic examination, measurement of keratometry, and a B-mode ocular ultrasound (Fig 1 ) with measurement of axial length. The implant calculation was done by the SRK-T formula and phacoemulsification was performed by the centurion® device. The average duration of follow-up was 15 months. Statistical analysis was performed by SPSS software, student's t-test was used to compare data between cases and controls, a p-value of <0.05 were deemed to be statistically significant.
6. Results
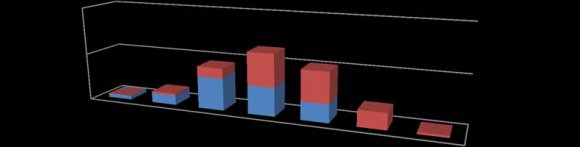
Regarding the results, the case group included 79 patients and the control group 80. The mean age in the case group was 59 ± 9.26 years and 69.82 ± 10.47 years for the control group, this difference was statistically significant (p: 0.001), for the distribution of patients according to the groups of age (Fig 2 ), we note the younger age of HM group (including subjects who underwent cataract surgery in their thirties), the majority were aged between 50 and 60 years, while for the control group most of the patients were aged between 60 and 70 years. In the HM group, men represented 40% compared to 50% in the control group. The best preoperative visual acuity was <1/10 in 82% of cases for severely myopic and in 75% of cases for the control population.
The mean axial length and power of IOL were 28.35 ± 1.77 mm and 6.27 ± 6.26 D (varying from -10 to 13 D), respectively, in the case group, and 22.76 ± 1.15 mm and 21.83 ± 2.52 D, respectively, in the control group (table1); 2: Intraoperative complications for the case and the control groups With regard to postoperative complications, there were 3 cases of retinal detachment, of which 2 eyes presented an intraoperative complication such as posterior capsular rupture, only 1 case of retinal detachment was identified in the control group. secondary cataract requiring the use of the YAG laser was more frequent in highly myopic eyes (32%) compared to the control population (23%), this difference was statistically significant (Table 3)
7. Discussion
High myopia is a risk factor for the onset of cataracts (7,8). Earliness of onset has been confirmed by numerous studies, generally 10 years younger than emmetrope. Our results match those of the literature [9,10], the average age of our highly myopic patients was 59 years compared to 69 years for the control group. A laboratory-based study identified a relationship between lipid peroxidation and myopic cataracts [11]. An animal study has also shown a correlation between the degree of retinal lipid peroxidation and lens opacity in rodents [12]. These studies provide a possible explanation for the association between high myopia and cataracts; damage to rodouter segments in high myopia results in products that induce cataracts.
In evaluating the highly myopic patient, several aspects apart from the routine cataract assessment should benoted. A detailed pastocular history is important, as previous refractive surgery, or intraocular contact lens or phakicintraocularlens implants, or retinal problems.
During the preoperative evaluation, the clinical examination must be rigorous to detect foreseeable intraoperative difficulties; special attention must be paid to the fundus analysis if the passage allows it. The calculation of the power of the implant is the second main issue in this preoperative assessment. It can be imprecise in the presence of a posterior staphyloma which requires an ultrasound measurement in B mode (13), the increments can pass to 1 diopter (D) in the low powers, in particular for implants with negative diopters (14), the refractive target must be well specified with the patients preoperatively, since some of them want to keep residual myopia and favor near vision without glasses.
For intraoperative difficulties, we find the higher risk of perforation during retro and peribulbar anesthesia (15), zonular fragility, the increase in the depth of the anterior chamber as well as the inverse pupillary block or the lens-iris diaphragmretropulsion syndrome: it corresponds to the retropulsion of the irido-cristalline complex during phacoemulsification, it is characterized by a deepening of the anterior chamber, a significant pupillary dilation and a concavity of the iris when the irrigation is introduced, it is due to the zonular fragility and to underdevelopment of the ciliary body of the highly myopic patients(14), this peculiarity complicates surgery by deepening the anterior chamber and causing pain to the patient.
In our series: the rate of posterior capsular rupture observed (7.5%) agrees with the results of the literature: varying from 2.8 for Zuberbuhler et al. (16) to 9.5% for Orchi et al. ( 17), slightly higher compared to the control group (5%).However, the difference between the group of cases and the control group was not statistically significant (p: 0.73). The use of YAG laser capsulotomy for secondary cataracts in highly myopic eyes ranges from 6.5% to 46.7% (21,22).in our series it was used in 32.9% of cases for HM, and 23.75% of cases for the control group. (p: 0.039) Indeed, the surgeon must face this challenge by adapting his surgical technique (23):
8. HM
-Concerning anesthesia, the topical one is quite feasible, a deeper anesthesia such as a sub-tenon or peribulbar often offers better operating comfort for the surgeon and the patient, -Prefer micro-incision <2.
9. Conclusion
Despite the modern techniques and technologies of cataract surgery, high myopia represents a challenge for surgeons at the different stages of treatment. It is essential to take pre-and intraoperative precautions, as well as postoperative monitoring.

| HM | Non-HM | p | |
| Axial length | 28,35 ± 1,77 | 22,76 ± 1,15 | P: 0.001 |
| Power of IOL | 6.27± 6.26 | 21,83 ± 2.52 | P: 0.001 |
| Peribulbar anesthesia was performed for 72 | |||
| patients, sub-tenon's anesthesia for 6 cases and | |||
| general anesthesia for 1 case. Intraoperative | |||
| complications represented 11% of our study group and | |||
| 7.5% of the control group. The difference between the | |||
| groups was not statistically significant ( | |||
| HM | Non-HM | P | |
| Retinal detachment | 3 | 1 | <0.001 |
| Secondary cataract | 26 | 19 | 0.039 |
| (yag) | |||
| implant decentering | 2 | 0 | 0.813 |
| IV. |
| Non-HM | P | ||
| Posterior capsular rupture | 7.5% | 5% | 0.73 |
| zonular dehiscence | 3.7% | 2.5% | 0.81 |
| anterior vitrectomy | 5,06% | 3.75% | 0.90 |
| No primitive implantation | 2,4% | 1,25% | 0.62 |
| Year 2020 |