1. Introduction
uberculosis is an infectious disease with high incidence and mortality rates in the world. Based on the World Health Organization (WHO) report in 2019, there is no single country free from Tuberculosis (TB).(1) Around 7 million Tuberculosis (TB) received treatment globally; however, the number of deaths was still hovering at 1.5 million patients. (2) Several factors that contribute to the high incidence of TB are sociocultural, including herbal medicines and stigma, adherence to drugs, TB program, and environment.(2)(3)(4)(5)(6) (7) The estimated incidence of TB cases in Indonesia is 845,000 cases per year, with 570,289 notified cases. Approximately 32% of cases have not been counted, either because they are not detected or not reported. (8) (9) Other than infected the lung, TB can also attack other organs such as bones, lymph nodes, and abdominal areas known as extrapulmonary tuberculosis (EPTB). (10) (11) The incidence of EPTB varies across regions ranging from 8% ?34% of all TB cases. Extrapulmonary tuberculosis (EPTB) levels vary widely -depending on their risk factors -including host immunological response, socio-demographics, comorbidities, lifestyle behaviors, genetic factors, and lymph node pathogenesis. (12) (13) It also depends on the previous history of pulmonary TB, non-adherence to taking anti TB drugs, and failure to therapy due to drug resistance.(3)( 14) Drugs of choice and inaccurate diagnoses depend on a country's socio-economic level and the resources devoted to the TB program.(2)(15) Direct sputum smear microscopy is the most widely used method for diagnosing pulmonary TB and is available in most primary health-care laboratories at the health-center level. Because TB can present with many different symptoms, the first obstacle in diagnosing smear-negative TB is discerning the varied clinical presentations. (13) (16) It is essential to determine which conditions are highly suspicious and included in the differential diagnosis. (17) (18) Previous studies have found that using a scoring system can support pulmonary TB diagnosis. (19) (20) This paper discussed the proposed scoring system for EPTB diagnostic tools based on several parameter discussed above. The data used for the parameters in the application were based on our study of 1,034 TB cases registered from 2015-2018 in Bandung.
2. II.
3. Approach
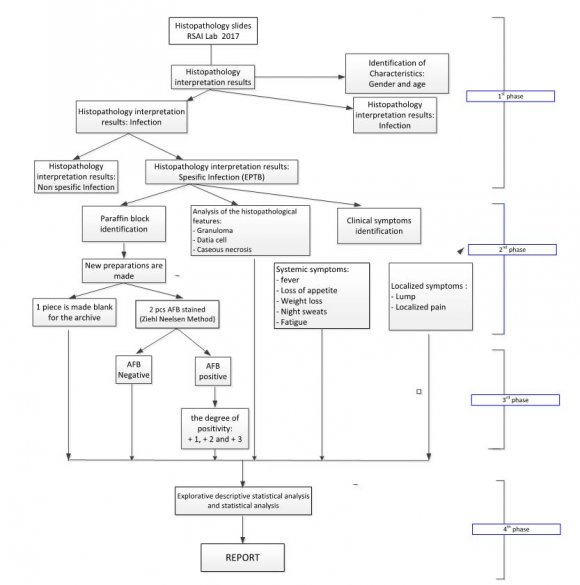
A diagnostic approach to an AFB smearnegative patient with possible TB includes, where available, a detailed medical history and clinical examination, as well as radiological, microbiological, molecular, and histological investigations. (21) Diagnosis of pulmonary tuberculosis in adults with clinical manifestations of chronic cough and sputum can be quickly made using the production of sputum smears with the Ziehl Neelsen AFB staining method. However, this method is challenging for the diagnose in patients with a non-productive cough that cannot expel phlegm and TB patients with HIV/AIDS or other immunecompromised conditions. ( 8 Below is the diagram showing the overall phase used in this study. Figure 1 taken initially from (21) described the approach used for the base of this study. F results. The results were presented according to the number of systemic manifestations and combined local manifestations and AFB and histopathological results. From 1,034 biopsied TB sputum smear using the AFB staining method and other supporting examination, we found 44 patients with EPTB, 3.4% of the total, which less than the average figure from the literature.
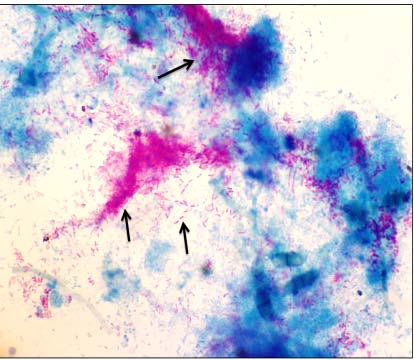
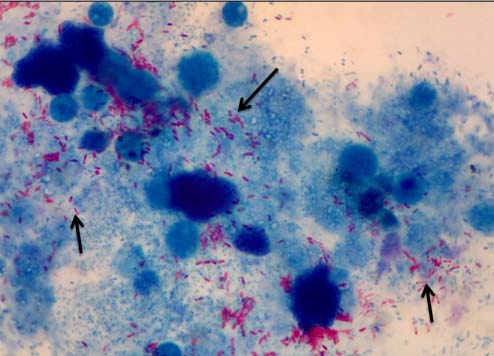
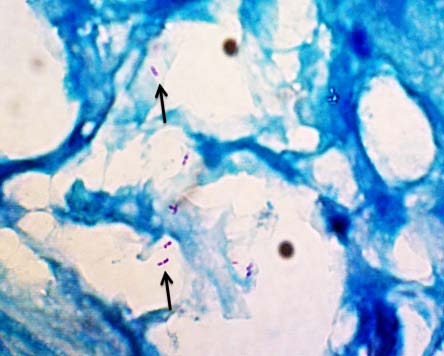
Positivity degree of EPTB recorded by AFB staining from paraffin block test preparations, using International Union Against Tuberculosis and Lung Disease (UATLD) scale modification on sputum smears.
AFB staining from the test material's sputum smear can be homogeneous, while the preparations from paraffin blocks cannot be homogenized because the test preparations come from different tissues. To accommodate those, the analysis of the data developed using two types of interpretation, some using the degree of positivity, and others used positive and negative findings only. EPTB based on the BTA count results and its relationship with systemic manifestations and local manifestations in EPTB patients is in the table below. Detected clinical manifestations in EPTB patients are divided into systemic manifestations and local manifestations. Systemic manifestations consist of fever, night sweats, fatigue, and weight loss. It appears that the number of patients who complain of fever is the same as those who complain of fatigue. Interestingly, the number of patients who complained of night sweats was the same as patients complained of weight loss. In addition to systemic clinical manifestations, there are also local clinical manifestations.
On these local manifestations, the symptoms depend on the origin of the organ where EPTB is located. Patients diagnosed with lymph node EPTB complain of enlarged lymph nodes accompanied by pain, while patients diagnosed with EPTB have lumps and pain. Overall, all EPTB patients complained of symptoms related to the origin of the organ where EPTB locate, although the number of complaints differed from patient to patient.
Most of EPTB occurred in the lymph nodes (48.6%), while the rest were evenly distributed among other organs, including bones, breasts, perianal, ileum. The findings were consistent with studies in other developing countries that have previously reported that the most frequent EPTB incidence location is in the lymph nodes (12)(13)(14)(15)(16). Histopathological readings from EPTB infection paraffin blocks found 97% of cases with granuloma (+); however, the AFB (+) was only 8.5%. It can be explained since granuloma collects several inflammatory cells, especially mature macrophages that form aggregates in response to an antigen. An antigen can come from a bacterium, a fungus, a foreign object, or an immune complex. The purpose of granuloma formation is to isolate the host body's antigen and facilitate the eradication of the antigen. Early in granuloma formation, antigen-presenting cells express a wide variety of proinflammatory and chemoattractant cytokines. The AFB staining results on the extrapulmonary TB patients' biopsy tissue based on the degree of positivity were mostly with a value of +1 (8.1%). There was no correlation between the degree of AFB's degree of positivity from biopsy tissue with clinical symptoms in this study.
Most EPTB sufferers do not experience systemic symptoms such as intermittent fever, night sweats, weight loss as experienced by TB patients in general. It is different from previous studies, which explained that systemic symptoms in EPTB patients were around 52.2% . (16) In this study, it was found that systemic fever complaints only occurred in about 16% of cases, night sweats in 5%, 5% experienced weight loss, 16% fatigue. In contrast, in the previous study, fever complaints were found in 37-80% of cases. ( 12) This study found that 100% of local clinical symptoms were statistically significant in patients with extrapulmonary TB based on the histopathological features and AFT staining with various positivity degrees. In contrast with previous studies, which explained that local symptoms in EPTB patients were only around 72%. (17) The histopathological examination results on the biopsy tissue were almost entirely with (+) granulomas since granuloma image is a characteristic feature of TB infected tissue. (15,18,19) There were no systemic clinical symptoms (97%) such as fever, night sweats, weight loss, and fatigue in patients with granuloma (+) features found on the histopathological result. In contrast with the other studies, which stated that the characteristic of TB infection histopathological is associated with the clinical manifestations of EPTB patients (15,(18)(19)(20)(21). Based on the above results and considering the scoring system that was previously used to enforce TB in children, a new scoring system is planned as an innovation to assist in diagnosing EPTB. This design expected to capture EPTB cases, taking into account several longused laboratory parameters found in this study. Other laboratory parameters will also support it as predictors of TB, such as erythrocyte sedimentation rates, monocyte/lymphocyte ratio, and neutrophil/lymphocyte ratio. (22)(23)(24) This scoring system's design uses a simple application that can be used using Android Studio since the aims are to use a broader community for EPTB case finding networking. (25) The simple design is chosen considering user ability on operating apps, which is relatively low. The "Extra-pulmonary TB Score Calculation System (EPTBScore)" application is an android based mobile application run on an android smartphone with a minimum android version of jelly bean 4.1. This system works by calculating the total score based on 22 parameters, as described in Table 3. In the application there are seven application pages, as follows:
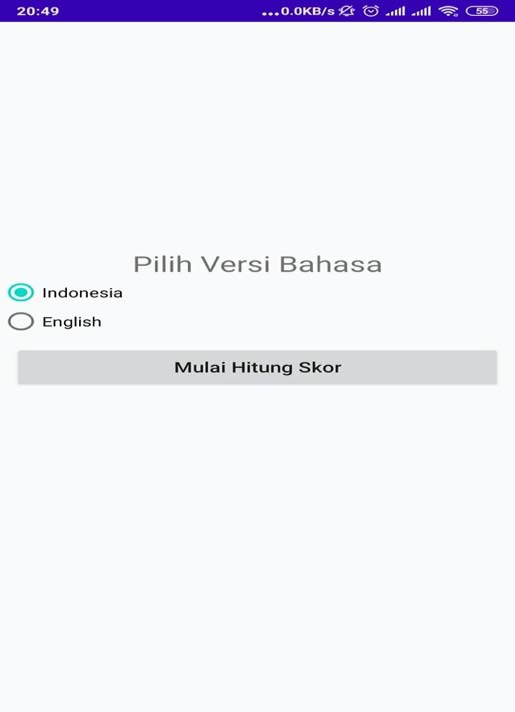
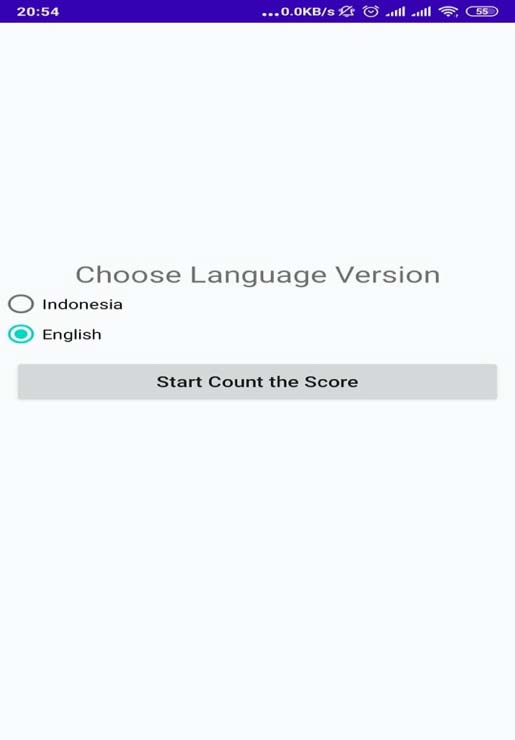
Opening Page; The opening page in the application only displays information of the the application name and originator. Figure 3 illustrates the opening page. The following pages will be for language preferences followed by pages for personal information such as name, age, and gender of the patient. The pages are illustrated in Figure The above proposed application designed to accommodate the need for several parameter inclusion. We developed a very simple application with regard to the user ability in operating application. This application is still in the development process with future plan of accomodataing user experience and needs.
4. III.
5. Conclusion
This paper presented the proposed EPTB Scoring Application used to diagnose Extrapulmonary Tuberculosis. The scoring system is ideal for accommodating many parameters from either systemic and local manifestation. Parameters chose using detailed medical history and clinical examination and radiological, microbiological, molecular, and histological investigations. It can also differentiate which conditions are highly suspicious and should be included in the differential diagnosis. EPTB Scoring system can be an alternative for EPTB diagnostic tools.

| Clinical | AFB stained | |||||||
| Manifestation | NA | ? | + | Total | ||||
| n | % | n | % | n | % | n | % | |
| Systemic | ||||||||
| Manifestation | ||||||||
| Fever | ||||||||
| Yes | 3 | 10 | 21 | 70 | 6 | 20 | 30 | 100 |
| No | 2 | 28,6 | 5 | 71,4 | 0 | 0 | 7 | 100 |
| Total | 5 | 13,5 | 26 | 70,3 | 6 | 8,1 | 37 | 100 |
| Weight Loss | ||||||||
| Yes | 4 | 11,4 | 25 | 71,4 | 6 | 17,2 | 35 | 100 |
| No | 1 | 50 | 1 | 50 | 0 | 0 | 2 | 100 |
| Total | 5 | 13,5 | 26 | 70,3 | 6 | 8,1 | 37 | 100 |
| Night Sweat | ||||||||
| Yes | 4 | 11,4 | 25 | 71,4 | 6 | 17,2 | 35 | 100 |
| No | 1 | 50 | 1 | 50 | 0 | 0 | 2 | 100 |
| Total | 5 | 13,5 | 26 | 70,3 | 6 | 8,1 | 37 | 100 |
| Fatique | ||||||||
| Yes | 4 | 11,4 | 25 | 71,4 | 6 | 17,2 | 35 | 100 |
| No | 1 | 50 | 1 | 50 | 0 | 0 | 2 | 100 |
| Total | 5 | 13,5 | 26 | 70,3 | 6 | 8,1 | 37 | 100 |
| Local | ||||||||
| Manifestation | ||||||||
| Yes | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 100 |
| No | 5 | 13,5 | 26 | 70,3 | 6 | 16,2 | 37 | 0 |
| Total | 5 | 13,5 | 26 | 70,3 | 6 | 16,2 | 37 | 100 |
| Year 2020 | ||||||||
| 34 | ||||||||
| Volume XX Issue XII Version I | ||||||||
| D D D D ) | ||||||||
| Global Journal of Medical Research ( | Clinical Manifestation Systemic Manifestation Fever Yes No Total Weight Loss Yes No Total Night Sweat Yes | No Granuloma n % 1 3,3 0 0 1 2,7 1 2,9 0 0 1 2,7 1 2,9 Histopathology Granuloma n % 29 96,7 7 100 36 97,3 34 97,1 2 100 36 97,3 34 97,1 | n 30 7 37 35 2 37 35 | Total | % 100 100 100 100 100 100 100 | |||
| No | 0 | 0 | 2 | 100 | 2 | 100 | ||
| Total | 1 | 2,7 | 36 | 97,3 | 37 | 100 | ||
| Fatique | ||||||||
| Yes | 1 | 3,2 | 30 | 96,8 | 31 | 100 | ||
| No | 0 | 0 | 6 | 100 | 6 | 100 | ||
| Total | 1 | 2,7 | 36 | 97,3 | 37 | 100 | ||
| Local Manifestation | ||||||||
| Yes | 0 | 0 | 00 | 0 | 0 | 0 | ||
| No | 1 | 2,7 | 36 | 97,3 | 37 | 100 | ||
| Total | 1 | 2,7 | 36 | 97,3 | 37 | 100 | ||
| PARAMETER |