1. Gestational Malaria and Factors Influencing Mosquito Bed Net use among Pregnant Women in Biyem-Assi, Yaounde
Judith Lum Ndamukong-Nyanga ? , Tchanga Chanceline Flore ? , Ngo Batandi Helen Virginie ? & Fegue Celestine ? Abstract-Malaria is an endemic parasitic disease in Cameroon and it is transmitted by the bite of the female Anopheles.
Malaria prevention methods are diverse. Their availability sometimes does not guarantee effective usage and the use of each method in isolation may not provide the necessary results for the fight against malaria. Pregnant women are relatively more vulnerable and so it is recommended that they should be protected against malaria. Proper protection will require the use of mosquito bed nets as major malaria prevention method. This study was designed to find out malaria prevalence and factors influencing the use of mosquito bet nets among pregnant women of Biyem-Assi Health District. Information on the knowledge of malaria and use of malaria prevention methods, especially bed nets was collected from 302 pregnant women attending prenatal clinics in health institutions within the Biyem-Assi Health District of Yaounde VI subdivision using a pretested questionnaire. Thick smear was prepared for screening Plasmodium parasites.
Analysis was done using EPI INFO version 16 (Chicago IL USA) and test of Chi 2. The study revealed that malaria prevalence was 48.5%. The shape of mosquito net had a significant (P = 0.05) effect on its use and a reduction on prevalence of malaria. The use of mosquito bed net was 47.7% while some of the women (52.3%) did not use it.
Profession significantly influenced (P ? 0.04) the use of mosquito bed nets. Some of the women did not use mosquito bed nets for different reasons such as heat, forgetfulness, neglect, dislike, etc. The shape and color influenced the use, but this was not significant. Use of mosquito bed nets as major malaria prevention methods is not considered as priority by pregnant women. Sensitization campaigns by government and NGOs should reduce malaria prevalence during pregnancy and give a priority position to mosquito bed nets.
2. Introduction
alaria is a fatal disease caused by parasites transmitted to humans through the bites of infected female Anopheles mosquitoes [1]. Its major impact is almost entirely on developing countries, especially in Africa [2]. More than 85% of malaria cases and 90% of malaria deaths occur in Sub-Saharan Africa and mostly during the rainy season [3].
In Africa, there are several risk factors for this disease. These factors are related to the existence of the vector that promotes the transmission of the parasite, in addition to the hot climate and low socio-economic conditions that have an impact on the control of the disease [4]. Vulnerable individuals include children under 5 years of age; unimmunized pregnant women, in whom malaria often leads to miscarriages, maternal deaths, low birth weight, abortions, stillbirths, and maternal anemia due to blood loss [5,6,7]; immunocompromised individuals; and international travelers from malaria-free areas. Pregnant women are more vulnerable because their immunity has been diminished by pregnancy [8].
In Cameroon, malaria remains the major endemic disease and one of the leading causes of morbidity and mortality in the most vulnerable groups [9]. According to the Cameroonian Ministry of Public Health, the disease accounts for 40 to 50 percent of the reasons for medical consultations, is responsible for 41 percent of deaths among children under five years of age, 18 percent of deaths in hospital facilities, and consumes about 40 percent of the annual household health budget [10]. The high morbidity and mortality rates can be explained by the insalubrity of the environment, anarchic constructions, ignorance by the population of prevention methods, low participation in control activities, lack of individual protection against mosquitoes, and the increasing resistance of plasmodium to usual antimalarial drugs [11]. With a view to reducing the spread of this disease, the efforts undertaken at the international level are relayed at the national level by a strong commitment of the State. Thus, through the Growth and Employment Strategy Paper (DSCE), the Cameroonian government has clearly stated the objective of reducing the death rate M associated with malaria to less than 10% by 2035 [12]. Thus, many measures have been taken, including free treatment and treatment of malaria.
Thus, many measures have been taken, including the free treatment of children under 5 years old suffering from uncomplicated malaria by all health facilities and the free distribution of several million longlasting insecticidal nets (LLINs) [13,14].
There is a gap between the acquisition of LLINs and their use as well as adherence to their use in families with pregnant women and children. Universal coverage of LLINs remains a major challenge in malaria prevention in Cameroon. For this study, the following specific objectives were developed : 1. To determine the prevalence of gestational malaria taking into account the socio-demographic characteristics of the participants in Biyem-Assi; 2. To determine the effect of bednet use on Plasmodium infection in pregnant women in Biyem-Assi; 3. To determine the factors influencing bednet selection and use by pregnant women in Biyem-Assi.
3. II.
4. Materials and Methods
5. a) Study Site
Yaoundé, the capital of Cameroon and capital of the Central Province is located 300 km from the Atlantic coast. It is surrounded by 7 hills, the highest of which are located on the West and North-West sides. Yaounde had an area of 13614 ha in 2002 and a population of about 2 million inhabitants in 2006. Its geographical boundaries are: to the west, the District of Mbankomo; to the east, the Division of Mefou-Afamba; to the south, the Division of Mefou-Akono; and to the north, the District of Okola [15]. The climate in the city of Yaounde is equatorial, characterized by the alternation of two dry seasons and two rainy seasons. The average temperature is 23.5 o C (with a range of 16 o C and 31 o C depending on the season), and rainfall is 1650 mm of water per year. The average air humidity is 80% and varies during the day between 35 and 98%. Frequent winds (humid) blow in a south-westerly direction; strong winds are oriented towards the north-west. The vegetation is of the intertropical type with predominance of southern humid forest [15].
6. b) Target population, Data and Sample Collection
The study population consisted solely of pregnant women receiving prenatal care (ANC) and who had voluntarily approved and signed the informed consent form. The criteria for non-inclusion were refusal to participate and failure to sign the informed consent form.
The sample size was calculated according to Lorentz's formula as follows:
N = (Z 2 ×P×Q)/d2where Z is the statistical power (1.96); P is the estimated prevalence of disease; 23% based on Tonga et al. 2013 [16]; Q=1-P; d represents the level of significance (0.05). Substituting into the formula gives N = 272 pregnant women.
To maximize sample collection and reliability of results, 350 women where issued consent forms and 302 gave consent and where enrolled in the study. Sample collection was carried out from July 25 to August 17, 2018.
7. c) Questionnaire
A pre-tested and validated questionnaire aimed at obtaining information on anthropometric, obstetric, environmental parameters and socio-demographic characteristics was given to each pregnant woman enrolled in the maternity ward. The information obtained was then recorded in a notebook, with a code assigned to each participant.
8. i. Collection of blood samples
The participant's code as well as the date was written directly on the slide. The finger was sanitized with an alcohol swab by massaging to stimulate blood circulation With a sterile lancet, the tip of the finger was pricked. By gently pressing the finger, two drops of blood were collected on the blade to be used for the thick film. The blood remaining on the finger was wiped off with absorbent cotton. With the corner of the second slide, the thick drop was made by bringing the two drops of blood together and spreading them in circular motion to form a uniform thick layer. The slides were air dried, stored in a slide box ready for staining.
9. d) Staining of thick film
Giemsa's dye was prepared from the stock solution. It was diluted at 1:20 (1 volume of Giemsa stock solution for 19 volumes of distilled water) and the mixture filtered through Whatman paper. The Giemsa was delicately poured into the staining trough until the slides were completely immersed. The slides were left to stain for 20 minutes. They were rinsed under running water. The slides were arranged to drain at an angle on a slide stand for 15 minutes for air drying.
10. i. Observation of slides
The slides were observed with the 100X objective (immersion objective) of the Light Microscope.
The thick film was used for the detection and quantification of trophozoites. The parasites were counted against 200 leukocytes and the Parasitemia (parasites/µL of blood) was calculated by considering an average of white blood cells at 8000/µL of blood for each individual according to the following formula: = ---------------------------------------------
11. Number of parasites counted × 8000 Parasitémie
12. Number of leukocytes (200)
Parasitaemia was considered low for parasite value < 500 / ?l blood, moderate for values between 501 -5000 parasites / ?l blood and high for parasite value > 5000 / ?l blood [17].
13. e) Statistical analysis
The data was entered into a work sheet using Microsoft® Excel 2010 and then analyzed using Epi Info? 7 (CDC, Atlanta). The association between bed net use as a preventive measure and sociodemographic factors was analyzed using the Chi-2 test. Frequencies were calculated and presented in tables and charts. The results were significant for a probability value P < 0.05.
14. f) Administrative and ethical considerations
Authorization was obtained at the University of Yaounde 1, signed by the Director of the school, the Head of Department of Biological Sciences and the Research Supervisor. Authorization and clearances were also obtained from the Ministry of Public Health Cameroon through the Directorate of the District Hospital of Biyem-Assi and through the Rector of the University of Yaounde I. An informed consent form was read and signed by the pregnant women. The information collected was treated confidentially. Only the members of the research team and the health personnel in charge of the follow-up of these women had access to it. Women carrying parasites were taken care of by the health care team at the health facility, in accordance with the recommendations of the dedicated control programs.
15. III.
Results and Discussion a) Results
16. i. Characteristics of the study population
A total of 302 pregnant women were enrolled in this study. The participants included in this study were predominantly Christian (295). They ranged in age from 17 to 53 with an average age of 25 ± 6 years. The majority of participants were students (89, 30.27%), single (169, 56.52%), and had a university education (147, 48.84%) (Table 1). The participants in this study generally had a good knowledge of malaria. Indeed, the majority had knowledge about transmission (94.79%), signs and symptoms (92.31%), consequences in children under 5 years of age (83.84%), knowledge on consequences of malaria in pregnant women (90.35%), dangers of malaria to society (88.10%), and preventive measures against malaria (97.93%) (Table 2).
Tableau 2: Knowledge on malaria transmission, consequences and prevention iii. Participants' perceptions of the net as a preventive measure against malaria For the participants' perceptions of the net, this study revealed that 22.33%, 33%, and 46.67% of participants rated the net (as a preventive measure against malaria) as excellent, very good, and good, respectively (Fig. 1).
17. Malaria prevalence among pregnant women
There was a high prevalence of gestational malaria found in the study population (48.5%). Women aged 25-34 years (48.45%), primiparous women (49.55%), those with a low level of education (60%), living in a poorly sanitized environment (presence of puddles, water and bushes: 50.35%) and being in their first trimester of pregnancy (58.49%) were the most affected by Plasmodium. The same was true for those living in wooden houses (50%). Regular use of the net decreased the prevalence of malaria among the pregnant women in this study although this difference was not significant (Table 3). Bed net ownership was influenced by the sociodemographic characteristics of the participants in this study. Bed net ownership was high among pregnant women aged 25-34 years (147, 48.7%), multiparous women (157, 52,0%), University students (84, 27,8%), and women with a higher levels of education (135, 44,7%) (Fig. 2).
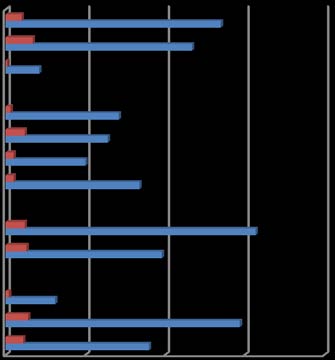
18. Possession of mosquito bednetsin relation to socio-demographic characteristics
19. No Yes
Participants' employment status significantly (P=0.04) influenced bed net ownership. Thus, students/pupils had high net ownership with a percentage of 31.23% compared to the formal/informal workers and housewives (26.39%, 23.79% and 18.59%, respectively) (Fig. 3).
20. vi. Effect of mosquito bed net use on Plasmodium infection in pregnant women
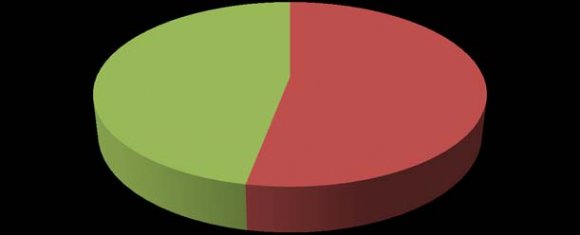
Participants who used the net had a Plasmodium infection rate of 53.49% (Table 4). Those using the rectangular shape were heavily infested with a prevalence of 50.37% compared to pregnant women using the white color (46.20%). The shape of the net significantly (P=0.05) influenced Plasmodium infection among participants (Table 4). The overall use of the net by pregnant women who participated in this study was 53%. (Figure 4). The choice of net was influenced by several factors. Pregnant women chose the net because it was spacious (39,74%), easy to install (41,72%), and comfortable and beautiful (18,52%) (Table 5). Several socio-economic factors of participants influenced net use, although this was not significant. Christian women, unmarried women, students, university students, and women aged 25-34 years had a higher rates of net use than their counterparts (Table 6). IV.
21. Discussion
Malaria in pregnancy is a major public health problem in sub-Saharan Africa. It poses a risk to both the mother and the fetus because it has a compromising effect on immunity in the latter [18]. Despite the poor implementation of malaria prevention strategies, their use has a reasonable effect on malaria and pregnancy parameters. Thus, gestational malaria is still a threat in our country. This study revealed a good knowledge of pregnant women on the causes and complications of malaria and the benefit of using preventive means such as the impregnated mosquito net, however the rate of net use was low.
The prevalence of gestational malaria has been reported throughout Africa and particularly in Cameroon [16,19]. The overall prevalence of gestational malaria is 48.5% in this study. This is higher compared to the 39.2% reported in the Mount Cameroon area. This may be due to poor compliance with malaria preventive methods; specifically the low use of the mosquito net which was 47.97% in the study conducted in Mount Cameroon [20]. This prevalence is very high compared to the 7.90% and 6.60% found among pregnant women living in rural [21] and urban [22] areas of Cameroon respectively. This result may be explained by the different study areas, the type of study or the use of Intermittent Preventive Treatment with Sulphadoxine-Pyrimethanin (IPT-SP). In rural areas, a prospective longitudinal study was conducted with a predominance of multiparous women in the study population.
The prevalence of malaria is higher in younger pregnant women although this is not significant. This has been similarly proven by previous studies conducted in the Littoral [16] and in South West Cameroon [19]. This is because this group of pregnant women have not yet acquired specific pregnancyrelated immunity that protects them from gestational malaria. This provides a better understanding of their susceptibility to Plasmodium falciparum. Consistent with previous studies, a poorly sanitized environment would influence the risk of malaria infection [19,23]. These authors report that proximity to fields and/or puddles increased the occurrence of malaria in pregnant women living in such environments.
Radio, television, and health centers were the main sources of information for the vast majority of participants in this study about malaria and its dangers. The majority of nets were obtained during prenatal visits. This finding is consistent with that conducted in Buea [24] where the primary source of nets for pregnant women had been ANC. The most recurrent shapes and colors were rectangular shapes and white colors, respectively.
Occupation agreement with that of Dionne-Odom reported in Cameroon. In addition, the net use rate was 47.67%. This rate is high compared to the 16.9%, 26%, and 17% observed in Cameroon [25,26], Nigeria [27] and Sub-Saharan Africa [28], respectively. A plausible explanation for this high net use could be the free net distribution campaigns by Cameroon's Ministry of Public Health (MINSANTE). In addition, the messages regularly disseminated through the various media channels always by this ministry on the use of the impregnated net as an effective means of malaria control have largely reached the populations. This is why the majority of our participants had heard about the net on television and radio. However, this rate of net use is low compared to that obtained in Buea (69.7%). Government action in easy accessibility justifies this proportion [24]. The shape of the net significantly influenced Plasmodium infection. The rectangular shape was the most used by participants in this study (268) for a malaria prevalence of 98.54% compared to 1.46% of infected participants using a conical shape net. This is because it is more spacious and fits the bed better. However, some participants preferred the conical shape because it was easier to install.
Given the high prevalence of malaria, net use is insufficient to significantly reduce malaria in this study population.
Cultural beliefs or prejudices are often cited as potential barriers to the adoption of innovative health behaviors and attitudes in Africa [29].. However, the results obtained in Cameroon indicate that, contrary to this idea, cultural beliefs are not the real explanatory factors for non-use of LLINs. This result is in agreement with those obtained in Niger [30]. However, education level is associated with net use. Women with at least secondary education had a high rate of net use. This result is due to the fact that those who have attained at least secondary school level are better able to read and understand messages on leaflets, radio, television. Thus, education remains an effective platform for influencing the behavior of pregnant women to reduce malaria prevalence.
In addition, net use by participants was significantly reduced by personal reasons such as heat, choking, burning, itching, and laziness to use the net. These findings corroborate those of previous studies conducted in North Cameroon [31] and Ghana [32], respectively, which reveals heat and choking sensation as reasons preventing net use by participants.
22. V. Conclusion and Recomendations a) Conclusion
This study revealed a high prevalence of parasitic infections (48.5%) in the study population.
Although not significant, the use of the net decreased the prevalence of malaria. However, the shape of the net significantly influenced Plasmodium falciparum infection.
Color and reasons such as heat, discomfort, suffocation, itching, fatigue, and odor influenced net use by pregnant women in the study. The color of choice for participants was white. Therefore, the shape and color of the net should be taken into account during distribution campaigns, as it affects not only the choice but also the use of the net. Awareness campaigns by the government and medical services would prioritize net use and significantly reduce the prevalence of the parasite malaria in this area.
23. b) Recomendations
In order to reduce morbidity and even death related to this parasitic disease, namely malaria, it would be wise for pregnant women to systematically sleep under a long-lasting impregnated mosquito net, despite the personal considerations and difficulties they have with regard to the latter.
Governments could adopt effective methods for reducing malaria prevalence such as Intensification of information, education and communication campaigns on malaria and its dangers among pregnant women.
In order to improve the use of impregnated mosquito nets, health officials should strengthen free distribution at health centers.
There is the need to increase awareness about the correct and regular use of the treated net;
The production of conical nets could be reduced to rectangular shapes and the white color could be the most predominant because it is the preference of pregnant women.
Author's contribution: JLNN Designed the work, participated in data collection, wrote and edited the manuscript, NBHV participated in data collection, data analysis and wrote the draft of the manuscript, TCF and FC contributed in data collection Declaration: All authors declare that there is no conflict of interest References Références Referencias
| Characteristic | Categories | Number of people | Prévalence (%) |
| Knowledge on mode of | Oui | 273 | 94,79 |
| transmission | Non | 15 | 5,21 |
| Recognition of signs and | Oui | 252 | 92,31 |
| symptoms | Non | 21 | 7,69 |
| Knowledge on the | Oui | 16 6 | 83,84 |
| consequences of malaria in | |||
| children from 0-5 years | Non | 32 | 16,16 |
| Knowledge on the | Oui | 206 | 90,35 |
| consequences of malaria in pregnant women | Non | 22 | 9,65 |
| Knowledge on the dangers | Oui | 222 | 88,10 |
| of malaria to society | Non | 30 | 11,90 |
| Knowledge on the | Oui | 284 | 97,93 |
| prevention and control of malaria | Non | 6 | 2,07 |
| iv. |
| Characteristic | Categories | No. Sampled | No. Infected | Prevalence (%) | ? 2 | P-valeur |
| ?25 | 101 | 49 | 48,51 | 1,23 | 0,74 | |
| Age (Years) | 25-34 | 161 | 78 | 48,45 | ||
| ?35 | 33 | 16 | 48,48 | |||
| Parity | Primiparous Multiparous | 111 169 | 55 80 | 49,55 40,70 | 0,05 | 0,81 |
| Trimester 1 | 53 | 31 | 58,49 | 4,46 | 0,10 | |
| Age of pregnancy | Trimester 2 | 126 | 53 | 42,06 | ||
| Trimester 3 | 120 | 61 | 50,83 | |||
| Students | 89 | 43 | 48,31 | 0,14 | 0,98 | |
| Profession | Housewives Formal workers | 55 74 | 27 35 | 49,09 47,30 | ||
| Informal workers | 76 | 35 | 46,05 | |||
| Level of education | ?Primary Secondary | 20 134 | 12 61 | 60,00 45,52 | 1,61 | 0,44 |
| University | 147 | 73 | 49,66 | |||
| Type of house | Wooden Block | 8 289 | 4 141 | 50,00 48,79 | 0,004 | 0,94 |
| Presence of bushes and | Yes | 143 | 72 | 50,35 | 0,15 | 0,69 |
| flowers around houses | No | 154 | 73 | 47,40 | ||
| ? |
| Characteristic | Category | Effectif No.sampled | No. Infected | Prevalence (%) | ? 2 | P-valeur | |
| Utilisation of mosquito bed | Yes | 258 | 123 | 53,49 | 0,29 | 0,58 | |
| nets | No | 43 | 23 | 47,67 | |||
| Form of the mosquito net | Conical | 9 | 2 | 22,22 | 1,74 | 0,05$ | |
| Rectangular | 268 | 135 | 50,37 | ||||
| White | 171 | 79 | 46,20 | 3,13 | 0,21 | ||
| Coulour of the mosquito bed net | Blue | 21 | 14 | 66,67 | |||
| Greeen | 2 | 1 | 50,00 | ||||
| ? 2 : Chi Square | P-valeur : level of significance | ||||||
| Factor | Number sampled | Prevalence (%) | ? 2 | P-valeur |
| Spacious | 120 | 39,74 | 4,46 | 0,18 |
| Easy to install | 126 | 41,72 | 0,06 | |
| Beautiful and comfortable | 56 | 18,54 | 1,11 | |
| Total | 302 | 100 |
| Characteristic | Categories | Number Sampled | Prevalence (%) | ? 2 | P-valeur |
| ?25 | 83 | 32,81 | 1,96 | 0,37 | |
| Age | 25-34 | 140 | 55,34 | ||
| ?35 | 30 | 11,86 | |||
| Marital status | Célibataire | 143 | 55,89 | 0,15 | 0,29 |
| Mariée | 113 | 44,14 | |||
| Chrétienne | 252 | 98,83 | 0,99 | 0,08 | |
| Religion | |||||
| Musulmane | 5 | 1,18 | |||
| Elève-Etudiante | 75 | 29,53 | 1,34 | 0,71 | |
| Ménagère | 50 | 19,69 | |||
| Profession | |||||
| Formel | 64 | 25,20 | |||
| Informel | 65 | 25,59 |