1. Introduction
arijuana also known as (Cannabis) or Cannabis Sativa, is a psychoactive drug from the cannabis plant used for medical and recreational purposes (1). It is one of the most commonly used psychoactive drugs worldwide, and it is one of the most popular illegal drugs (2). Main psychoactive part of cannabis is tetrahydrocannabinol, which has a scientific name called "Cannabinoids and Cannabidiol. Cannabinoids are usually classify as endocannabinoids, phytocannabinoids, and synthetic cannabinoids. Synthetic cannabinoids are in the gathering of drugs called new psychoactive substances and these technically synthetic cannabinoid receptor agonists are designer drugs that mimic the psychoactive effects of cannabis (3). There is a long tradition of cannabis use for culinary, medicinal and ,ceremonial purposes in many developing countries. Various intake routes of tetrahydrocannabinol THC (intravenous, smoke, inhalation and, oral) so can be used by smoking, vaporizing, in food, or an extract. The plasma levels are related to onset, degree and duration of clinical effects. The degree of response and plasma cannabinoid levels attain edvary in a dose-related manner depending upon the potency of smoked marihuana (4). Over the last decades, there have been considerable researches involving cannabinoids and their importance in regulating a variety of physiological M and psychological processes such as pain, feeding behavior, lipid metabolism, pleasure sensation, and immune system (4). The physical harm caused by cannabis is less well-known. In adults, chronic bronchitis, lung cancer, myocardial infarction, hepatotoxicity, decreased sperm count and motility, gynecomastia in males, suppression of ovulation among females, low birth weight and delayed visual system, and development among the newborns of cannabis using females (3). Plant-derived cannabinoids include delta-9-tetrahydrocannabinol (THC), the primary psychoactive component of cannabis. Cannabinoids mediate their effects through binding specific receptors, which are members of the G protein-coupled receptor superfamily. Two cannabinoid receptors was identified: Cannabinoid-1 receptor (CB1) and cannabinoid-2 receptor (CB2). CB1 is expressed primarily in the central nervous system (CNS) and is responsible for the psychoactive effects of cannabinoids by modulating neurotransmitter release). In contrast, CB2 is localized primarily in immune cells such as lymphocytes, macrophages, and neutrophils and is responsible for the immunomodulatory effects of cannabinoids (5). Smoking is the most important health problem in the world. Many studies proved its harmful effects on many organ systems like respiratory, reticuloendothelial system, and cardiovascular systems. ( 6) Tobacco cigarette smoking is one of the main leading causes of death worldwide. Continuous cigarette smoking has severe adverse effects on hematological parameters (e.g., hemoglobin, white blood cells count, mean corpuscular volume, mean corpuscular hemoglobin concentration, red blood cells count, hematocrit). These represented a predisposing factor for the development of various pathological conditions, and diseases such as atherosclerosis, polycythemia vera, chronic obstructive pulmonary disease and cardiovascular diseases. (7) Smoking effects on hematological indices observed on routine complete blood count testing (CBC). Smoking-induced increased in red blood cell count (RBC) was described. Current smoking has been reported as an associative factor with leukocytosis (TLC), thrombocytosis (PLTS) in some reports. Nicotineinduced JAK-STAT &NF-Kb signaling pathways are thought to mediate the increase in RBC. (8) II.
2. Materials and Methods
Study population: Sudanese voluntary cannabis abusers and Cigarette smokers in Khartoum state, Sudan.
Inclusion criteria: This study included Sudanese voluntary cannabis abusers and Cigarette smokers in Khartoum state, Sudan.
Exclusion Criteria: The Participant with any disease or smoking any other type of smoking was excluded.
Data collection: Collected using self administrated per coded questionnaire, which was specifically designed to obtain information to this study.
Blood sampling: Venous blood was collected using sterile disposable plastic syringes after cleaning the venous puncture area with 70% ethanol, the blood 2.5 ml was added to the anticoagulant container EDTA.
3. Methods:
The result was calculated by CBC analyzer. Whole blood is passed between two electrodes through apertures so narrow that only one cell can pass through at a time.
Statistical Analysis: Statistical assessment was carried out with statistical package for social sciences (SPSS) version 17.0 for windows statistical software.
Ethical Considerations: All participants were voluntarily submitted written informed consent before the commencement of the study. Neither the participant name nor situation or any other information was used in this study.
4. III.
5. Results
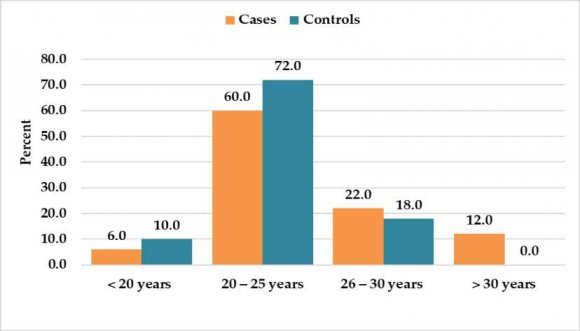
A total of 100 Sudanese participants were enrolled in our research, divided into 50 Sudanese individuals smoking cannabis plants as a case group and 50 healthy Sudanese individuals as a control group. (Fig. 1). All study participants were males with ages ranged from (17) to (35) years old in both groups. (Fig. 2). Concerning some other Cannabis smoking characteristics, the majority of cases group 38 (76%) reported smoking duration more than three years and almost nearly all of them, 49 98%, reported smoking frequencies of more than five times per week as detailed in figure (3), and Table (1). In regards to the effect of cannabis smoking on the results of complete blood count test results, our study showed that measures of cases group were significantly higher among cases group compared to the control group in white blood cells count (p = 0.0121), HCT (p = 0.0055), neutrophil count (p = 0.0428) and in RDW -SD (p = 0.004). The study showed that measures of the cases group were significantly lower among case group compared to control group in platelets count (p = 0.0477), and in the Lymphocytes count (p = 0.0238) as detailed in the table (2). Lastly, the study did not find a significant difference in the complete blood count measures according to the duration of cannabis smoking among the case group except in hematocrit (p = 0.041) as detailed in Table (3) the study was not able to assess the effect of cannabis smoking frequency/week of the measures of complete blood count because of the lack of variation in the relevant data; because all most all 49 (98%) of the case group had a similar frequency of weekly cannabis smokers. Among the cigarette smokers this study showed that the majority, 36 72% of the cases group (smokers) were within the age group 20 -25, as detailed in Table (4). Concerning some other smoking characteristics, more than half of cases group 27 (54%) reported smoking cigarette duration less than five years, and almost the majority of them, 40 80% reported smoking frequencies less than ten times per day as detailed in Tables 5 and 6. In regards to the effect of cigarette smoking on the results of complete blood count measures, our study showed that results of cases group were significantly higher among cases group compared to control group in mean cell volume (p = 0.0362), in PWD (p = 0.0259) as detailed in Table (7) Moreover, the study did not find a significant difference in complete blood count measures according to the duration of smoking among case group except in white blood cells count (p = 0.0419) as detailed in Table 8. This study did not find a significant difference in complete blood count measures according to the frequency of smoking among case group except in white blood cell count (p = 0.0473) as detailed in Table (9).
6. Discussion
The effect of Cannabis "marihuana" on hematological parameters has been discussed by many authors as it is the most popular illegal drug used worldwide. This study had demonstrated the effects of cannabis abusing and Cigarette smoking on some hematological parameters, including 100 Sudanese participants, divided into 50 Sudanese individuals smoking cannabis plants as the case group and 50 healthy Sudanese individuals as the control group. Our study revealed a significant higher increase in the WBCs, HCT, absolute neutrophil count and RDW-SD, with P.values equal= (0.012), (0.005), (0.04) and (0.0004) respectively. The WBCs count was higher in case group (mean=6.26) cell/?l compared with control group (mean=5.20) cell/?l. This result was agreed with Deryas study (8) and disagreed with Amaechi and his colleagues study (6). Also, HCT showed a statistically significant higher difference between the case group and the control groups, in which the mean in case group was (46.6) % and (43.2) % in control group. Our result disagreed with the study carried in Nigeria by Amaechi and his colleague which showed lower HCT (6). The mean of Neutrophils absolute count in the case group was (2.5) cell/?l compare with (1.88) cell/?l in the control group. Our result was agreed with stud carried by Derya (8) and disagreed with the studies carried by Amaechi (6) and Salma studies (7). While the brilliant highly significant difference in the mean of RDW-SD in case group, which equal (44.7) fl was higher compare with control group (42.4) fl. This result was agreed with findings of the Derya study that their study showed a significantly increase in RDW-SD (8). On the other hand, our study revealed a significant lower difference in platelete count and lymphocyte percentage count with Values equal (0.04) and (0.02), respectively. Which agreed with the studies carried out by Amaechi (6) and salma (7). While the insignificant differences of RBCs (P.Value=0.35) were agreed with Salma, Amna and, Bashiri studies (7,9,10). Also, Hb concentration revealed no significant difference between both groups with P. Value (0.42) which agreed with Amna, Bashiri and, Derya studies (10). All studies agreed with our findings revealed no significant difference on RBCs indices; MCV, MCH, MCHC, MPV, PDW and P-LCR. Differences in our findings from previous studies may be attributed to the racial, genetic, geographic, nutritional status, duration of cannabis abusing and differences in sample size included. (8,9). Among Sudanese cigarette smokers, our result showed that measures of CBC were significantly higher among the cases group compared to the control group in mean cell volume (p = 0.0362), and in PDW (p = 0.0259) and the duration of smoking and its frequency significantly increase white blood cells count (p = 0.0419), (p = 0.0473) respectively. Our result revealed that there was a significant increase in MCV and this finding disagree with Naser M Ergiah,et al, Rawia O. A Mustafa and Muhammad Asif,et al finding that showed there was no significant difference in MCV.( 14) (15) (17) Similarly, we found that there was a significant increase in PDW in among smokers compared to non-smokers and these findings disagree with Muhammad Asif, et al. Findings which show that did not show any significant difference in PDW. ( 17) Furthermore, our result stated that there was no significant difference in MCH, RDW, PLT, MPV and this result agree with Muhammad Asif, et al findings which show that it did not show any significant difference in MCH, RDW, PLT, MPV. (17). On the other hand, our result showed no significant difference in WBCs, RBCs, Hb and ,MCHC and this disagree with Naser M Ergiah,et al findings that stated there was a significant increase in these parameters.( 14) Also, our result reported that there was no statistically significant difference in total WBCs and, platelets count and this result disagrees with Dinesh et al which their results show there was a slight increase in white blood cells (WBCs) and platelets observed in smokers compared with non-smokers. (13). We found that there was no statistically significant difference in MCH and PLT and this findings agreed with Naser M Ergiah, et al result. (14) . Similarly, we found that there was no statistically significant difference in RBCs, HB, HCT, MCH, RDW-SD, RDW-CV, Neutrophils, Monocytes and, Eosinophils. And this result disagrees with Rawia O. A Mustafa finding that stated a significantly increase in these parameters and Muhammad I. Khan, et al result which reported that Hemoglobin, RBC Count, HCT and MCH were significantly increased. (15) (16). Furthermore, we found that there was no significant difference in PLT count and these finding disagrees with Rawia O. A Mustafa finding that showed there was a significant decrease observed in PLT count. (15). Finally, we found no significant difference in WBC, RBC, Hb, HCT, MCHC and PCT and, this result disagrees with Muhammad Asif, et al findings which show that WBC, RBC, Hb, and HCT were significant high, at the same time MCHC and PCT were significantly low. (17) V.
7. Conclusion
Our study concluded that some hematological parameters in cannabis smokers differ significantly from non-smoker ones. The most likely consequences are an increase in TWBCs count, HCT, Neutrophils absolute count and, RDW. Also, the study revealed that cannabis abusing results in a low level of platelet count and lymphocyte percentage count., there was no change in RBCs count, Hb concentration, MCV, MCH, MCHC, MPV, PDW and ,P-LCR. Among Sudanese cigarette smokers, the study concluded that smoking might result an increase of MCV and PDW and, long smoking duration and high frequency per day may lead to high

| RDW-SD (%) | 44.73 | 42.41 | 2.31 | 0.0004 | |||
| Cannabis smoking frequency -week RDW-CV (%) 13.58 | Frequency 14.11 | -0.53 | Percent (%) 0.0833 | ||||
| < 5 times / week | 1 | 2.0 | |||||
| PDW (%) | 16.85 | 15.80 | 1.05 | 0.0819 | |||
| > 5 times / week | 49 | 98.0 | |||||
| MPV (fL) | 11.20 | 10.95 | 0.26 | 0.6012 | |||
| Total | 50 | 100.0 | |||||
| Year 2021 | P-LCR (fL) PCT (ng/ml) | 27.14 Table (2): The difference in complete blood count results between the study groups 27.33 -0.19 (n = 100, 50 cases + 50 controls). Study groups 0.25 0.29 -0.03 | 0.8557 0.0777 | ||||
| 18 | |||||||
| Volume XXI Issue III Version I | Complete blood count WBC (× 10 3 ) RBC (× 10 3 ) HGB (g/dL) HCT (%) | Mean in Case 6.26 5.45 14.36 46.62 | Mean in Control 5.20 5.24 14.04 43.29 | Difference 1.07 0.21 0.32 3.33 | P value 0.0121 0.3539 0.4234 0.0055 | ||
| D D D D ) | MCV (fL) | 84.48 | 82.15 | 2.33 | 0.2855 | ||
| ( | |||||||
| Medical Research | MCH MCHC (g/L) PLT (× 10 3 ) | 27.78 35.19 237.06 | 26.95 32.68 269.44 | 0.83 2.51 -32.38 | 0.1231 0.4774 0.0477 | ||
| Global Journal of | LYM (× 10 3 ) NEUT(× 10 3 ) MIX (× 10 3 ) | 2.22 2.50 1.16 | 2.15 1.88 1.13 | 0.07 0.63 0.03 | 0.7814 0.0428 0.8482 | ||
| LYM (%) | 35.88 | 42.08 | -6.20 | 0.0238 | |||
| NEUT (%) | 39.18 | 36.35 | 2.83 | 0.4033 | |||
| MIXD (%) | 18.91 | 20.20 | -1.29 | 0.6402 | |||
| Evaluation of Blood Elements and Red Blood Cell Indices among Sudanese Cannabis and Cigarette | |||||||
| Smokers in Khartoum State | |||||||
| MIXD (%) | 20.18 | 18.31 | 19.07 | 18.91 | 0.811 | ||
| RDW-SD (%) | 45.10 | 44.77 | 44.15 | 44.73 | 0.525 | ||
| RDW-CV (%) | 14.26 | 13.19 | 13.88 | 13.58 | 0.582 | ||
| PDW (%) | 16.31 | 16.85 | 17.51 | 16.85 | 0.309 | ||
| MPV (fL) | 12.83 | 10.55 | 11.08 | 11.20 | 0.177 | ||
| Year 2021 | P-LCR (fL) PCT (ng/ml) | 25.95 0.28 | 27.39 0.23 | 27.86 0.28 | 27.14 0.25 | 0.379 0.923 | Year 2021 |
| 20 | 19 | ||||||
| Volume XXI Issue III Version I | Complete Blood Count WBC (× 10 3 ) (CBC) RBC (× 10 3 ) HGB (g/dL) | Duration of Cannabis smoking (years) < 3 3 -5 > 5 6.36 6.20 6.33 5.35 5.23 6.17 14.75 14.19 14.38 | Overall mean 6.26 5.45 14.36 | P value 0.967 0.241 0.692 | Volume XXI Issue III Version I | ||
| D D D D ) I | D D D D ) | ||||||
| ( | HCT (%) | 50.41 | 45.61 | 44.91 | 46.62 | 0.041 | ( |
| Medical Research | MCV (fL) MCH MCHC (g/L) | 81.68 27.67 46.02 | 84.24 27.64 31.72 | 88.51 28.32 31.91 | 84.48 27.78 35.19 | 0.236 0.577 0.163 | Medical Research |
| Global Journal of | PLT (× 10 3 ) LYM (× 10 3 ) NEUT(× 10 3 ) | 243.17 2.32 2.04 | 228.04 2.02 2.59 | 255.00 2.65 2.82 | 237.06 2.22 2.50 | 0.792 0.676 0.327 | Global Journal of |
| MIX (× 10 3 ) | 1.14 | 1.14 | 1.25 | 1.16 | 0.776 | ||
| LYM (%) | 36.23 | 33.11 | 43.21 | 35.88 | 0.374 | ||
| NEUT (%) | 35.08 | 40.25 | 41.12 | 39.18 | 0.391 | ||
| © 2021 Global Journals | |||||||
| Duration of smoking | |||||||||
| (years) | |||||||||
| Complete blood count Complete blood count | Study group | Difference Overall mean | P value P value | ||||||
| < 5 | 5-10 | > 10 | |||||||
| Case | Control | ||||||||
| WBC (× 10 3 ) WBC (× 10 3 ) | 5.38 4.11 | 5.22 | 5.10 | 6.58 | 0.28 | 5.38 | 0.3340 0.0419 | ||
| RBC (× 10 3 ) RBC (× 10 3 ) | 5.24 5.29 | 5.17 | 5.22 | 5.25 | 0.02 | 5.24 | 0.7970 0.5110 | ||
| HGB (g/dL) HCT (%) HGB (g/dL) HCT (%) | 14.06 43.08 14.10 43.46 | 13.91 42.48 14.13 42.83 | 13.45 41.73 | 0.15 0.60 | 14.06 43.08 | 0.5760 0.3547 0.4020 0.1730 | Year 2021 | ||
| MCV (fL) MCV (fL) | 82.61 82.67 | 77.20 83.14 | 79.70 | 5.41 | 82.61 | 0.0362 0.5610 | |||
| Volume XXI Issue III Version I D D D D ) | MCHC (g/L) PLT (× 10 3 ) LYM (× 10 3 ) NEUT (× 10 3 ) MIX (× 10 3 ) LYM (%) MCH (pg) MCH (pg) MCHC (g/L) PLT (× 10 3 ) LYM (× 10 3 ) MIX (× 10 3 ) NEUT (× 10 3 ) | 27.04 32.69 263.86 2.20 0.73 2.49 6 41. 4 26.96 32.54 266.74 2.12 0.67 2.59 | 26.84 32.67 278.52 2.10 0.75 2.25 41.68 27.43 32.99 262.37 2.41 0.84 1.96 | 25.73 32.28 251.50 1.68 0.57 4.33 | 0.20 0.02 -14.66 0.09 -0.02 0.24 -0.04 27.04 32.69 263.86 2.20 0.73 2.49 | 0.6957 0.9353 0.3274 0.4726 0.7940 0.3236 0.9854 0.6360 0.9810 0.7550 0.6480 0.5760 0.4640 | Volume XXI Issue III Version I D D D D ) | ||
| Medical Research ( | MIXD (%) NEUT (%) RDW-CV (%) RDW-SD (%) PDW (%) MPV (fL) P-LCR (fL) PCT (ng/ml) MPV (fL) RDW-CV (%) RDW-SD (%) PDW (%) LYM (%) MIXD (%) NEUT (%) | 13.71 44.43 14.08 42.78 16.78 11.23 28.30 0.29 11.41 14.11 43.06 16.84 40.08 12.57 46.61 | 15.11 42.37 16.26 42.34 15.59 12.71 26.81 0.29 11.01 14.02 42.69 16.56 46.57 16.33 37.37 | 11.05 14.13 41.28 17.38 28.78 8.98 63.25 | -1.40 2.06 -2.18 0.44 1.19 -1.48 1.49 0.01 | 11.23 42.78 16.78 14.08 41.64 13.71 44.43 | 0.4214 0.4397 0.3119 0.0259 0.4458 0.1019 0.1730 0.7018 0.6190 0.9280 0.1140 0.3973 0.6810 0.7870 0.8560 | Global Journal of Medical Research ( | |
| P-LCR (fL) | 29.04 | 27.38 | 27.65 | 28.30 | 0.0840 | ||||
| PCT (ng/ml) | 0.30 | 0.29 | 0.27 | 0.29 | 0.2690 | ||||
| © 2021 Global Journals | |||||||||
| Complete blood count | Frequency of smoking (daily) | Overall mean | P value | ||
| < 10 | ? 10 | ||||
| WBC (× 10 3 ) | 4.27 | 6.01 | 5.38 | 0.0473 | |
| RBC (× 10 3 ) | 5.27 | 5.13 | 5.24 | 0.3669 | |
| HGB (g/dL) | 14.12 | 13.80 | 14.06 | 0.3188 | |
| HCT (%) | 43.31 | 42.18 | 43.08 | 0.2127 | |
| MCV (fL) | 82.65 | 82.45 | 82.61 | 0.9104 | |
| Volume XXI Issue III Version I | MCH (pg) MCHC (g/L) PLT (× 10 3 ) LYM (× 10 3 ) MIX (× 10 3 ) | 27.06 32.69 268.55 2.23 0.71 | 26.99 32.73 245.10 2.07 0.82 | 27.04 32.69 263.86 2.20 0.73 | 0.9342 0.9085 0.4955 0.2790 0.3690 |
| D D D D ) I | NEUT(× 10 3 ) | 2.54 | 2.28 | 2.49 | 0.5985 |
| ( | |||||
| Medical Research | MIXD (%) NEUT (%) LYM (%) | 13.11 44.52 42.10 | 16.11 44.08 39.82 | 13.71 44.43 41.64 | 0.1775 0.9267 0.5710 |
| RDW-CV (%) | 14.12 | 13.91 | 14.08 | 0.0932 | |
| RDW-SD (%) | 42.98 | 41.99 | 42.78 | 0.1453 | |
| PDW (%) | 16.74 | 16.94 | 16.78 | 0.7147 | |
| MPV (fL) | 11.23 | 11.21 | 11.23 | 0.9414 | |
| P-LCR (fL) | 28.34 | 28.13 | 28.30 | 0.8401 | |
| PCT (ng/ml) | 0.30 | 0.27 | 0.29 | 0.1809 | |
| © 2021 Global Journals | |||||