1. Introduction
ractures of the distal radius are the most common fractures accounting about one sixth of the total skeletal injuries 1. As high as 40% to 49% are considered to be unstable that requires surgical fixation. 2 Most functional tool for the physical activity of human being is "the hand". Improper treatment of unstable distal radial fracture, may compromise hand function. 3 Management of the distal radius fractures are dictated by the pattern of the fractures, degree of displacement of the bone fragments, involvement of the fracture with the joints, associated soft tissue injuries, and the patients pre-injury activity level and physical demands. 4 Unstable distal radius fracture requires surgical fixation of the broken bone because closed reduction (non-surgical manipulation and casting) often is insufficient to maintain fracture reduction and promote bone healing. Operative management of the distal radius fracture has been studied extensively and has evolved over past decade. The best treatment of unstable distal radial fracture is not well established. So, the treatment of unstable distal radial fractures continues to improve as better method of fixation and soft tissue management are more to be developed. 5 With the locking system, distal screws are locked to the plate, which stabilizes the screws against lateral movement (toggle effect). This provides augmentation to the strength of fixation by producing "single bone-plate-screws construct" which producing a scaffold in the mostly cancellous distal radial metaphysis & also under distal radial articular surface.
This new technique of fixation is now sporadically being practiced in Bangladesh: For "A good Functional hand", the use of "Volar locking plating system" may be considered as a better tool in the treatment for unstable distal radial fractures in ourcountry.
2. II.
3. Objective
? To evaluate the outcome of surgical management for unstable fracture of the distal radius by volar locking plating system.
III.
4. Methodology
Type of study: This is an observational prospective clinical study.
Place and period of study:
5. Inclusion criteria
? Unstable fracture of distal radius.
? Closed or open with soft tissue injury (Gustillo I & II)
? Age-any adult patient.(18-70 years)
Exclusion criteria
? Open fracture (Gustillo type III)
? Stable fracture.
? Undisplaced fracture.
? Acute medical illness.
? Poly traurna patient.
? Patients with mental or psychic issues.
6. Sample selection
A total of 30 Patient attended at Emergency Department and OutpatientDepartment of Chittagong Medical College hospital & PrivateHospital in Chittagong were selected considering the inclusion criteria.
IV.
7. Results
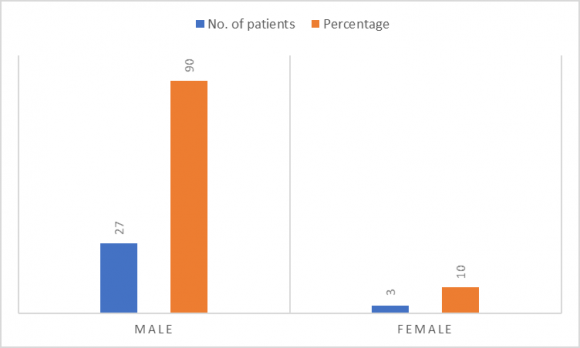
In In figure-1 shows gender distribution of the patients where 90% patients were male and 10% patients were female. The following figure is given below in detail: In table-2 shows distribution of the patients according to side affected where most of cases were left side were affected, 56.7%. The following table is given below in detail: In table-7 shows distribution of incidence of complications where 13.3% patients had wrist stiffness followed by 10% had persistent wrist pain and reduced grip strength, 3.3% had surgical site infection and late collapse. The following table is given below in detail:
8. Discussion
There were some complications in this study. Two case developed tourniquet palsy in immediate postoperative period but fully improved within few days. Once case had feature of late collapse though fixed properly earlier. Wrist stiffness was in 4 cases which improved but not significantly after physiotherapy. Persistent wrist pain developed in one case.
Step off>2mm seen in one case.
Correction and maintenance of anatomical land mark (radial length, radial angle, and dorsal angle) are the most important factors to regain hand and wrist function. Anatomical and functional outcome in this was good to excellent in most of the cases.
The volar locking plating system as a method of fixing distal radius fracture has been shown one of the effective methods in relation with anatomical and functional outcome of the wrist joint. An advantage of the volar plating technique is the comfort that it provides to patients in initiating early finger and wrist motion. 6 The locking screws in the volar locking plating system offer and additional advantage over previous implants. 7 With previous volar plate designs involving non-locking screws, screw purchase in the metaphysis of the distal part of the radius often was poor because of the limited amount of cortical bone in this location. With the new design, the distal screws are locked to the plate, which stabilizes the screws against lateral movement (toggle) and resists loosening. 4 This provides additional strength to the fixation by constructing a scaffold under the distal radial articular surface and producing 'bone-plate-screws construct'. 8 Plate-related complications did not occur in this series. The pronator quadratus provided muscular coverage of the plate and shielded the flexor tendons from the plating system.
In this study average follow-up period was 6 months. The mean Gartland and Werley score improves significantly from 4 points at 6 months to 2 points at two years. 9 Male attended more for 'Volar Locking Plating System expecting good functional hand for the cost of procedure.
9. VI.
10. Conclusion
Management of distal radius fracture for adult patients with volar locking plating system results in satisfactory outcomes in most of the cases with minimum complications.
| Study population: |
| Age group | No. of patients | Percentage |
| 18-30 | 9 | 30 |
| 31-45 | 17 | 56.7 |
| 46-70 | 4 | 13.3 |
| Total | 30 | 100 |
| Table-3: Time intervals between injury and management | ||
| Time Interval | No. of Patients | Percentage |
| 1-3 | 11 | 36.7 |
| 4-7 | 08 | 26.7 |
| 8-14 | 09 | 30.0 |
| 14-20 | 02 | 6.6 |
| Total | 30 | 100 |
| In table-4 shows distribution of associated injuries where 3.3% had fracture SOF. The following table is given | ||
| below in detail: | ||
| Table-4: Distribution of associated injuries | ||
| Associated injuries | No. of patients | Percentage |
| Fracture SOF | 1 | 3.3 |
| Fracture trochanter of femur | 0 | 0 |
| Fracture NOF | 0 | 0 |
| Chest Injury | 0 | 0 |
| Side Affected | No. of patients | Percentage |
| Right | 13 | 43.3 |
| Left | 17 | 56.7 |
| Total | 30 | 100 |
| Hospital stay (day) | No. of patients | Percentage |
| 1-2 | 0 | 0.0 |
| 3-4 | 22 | 73.3 |
| 5-6 | 05 | 16.7 |
| 7-8 | 03 | 10.0 |
| Total | 30 | 100 |
| In table-6 shows Distribution of outcome of physiotherapy. 23.3% cases were excellent followed by 60% | ||
| cases were good, 10% cases were fair, 6.7% cases were poor. The following table is given below in detail: | ||
| Table -6: Distribution of outcome of physiotherapy | ||
| Result | No. of Patients | Percentage |
| Excellent | 7 | 23.3 |
| Good | 18 | 60.0 |
| Fair | 3 | 10.0 |
| Poor | 2 | 6.7 |
| Total | 30 | 100 |
| V. | ||
| 7: Distribution of incidence of complications | ||
| Complications | No. of Patients (total=15) | Percentage |
| Persistent wrist pain | 3 | 10.0 |
| Wrist stiffness | 4 | 13.3 |
| Finger stiffness | 0 | 0.0 |
| Reduced grip strength | 3 | 10.0 |
| Reduced pinch power | 0 | 0.0 |
| Surgical site infection | 1 | 3.3 |
| Late collapse | 1 | 3.3 |