1. Obesity and its Relation to Coronary Artery Disease (CAD) Incidence
Lt Col Md Fakhrul Alam ? , Dr. Israt Jahan ? , Dr. Md. Ataul Hoque ? , Capt Swapnil Kumar Roy ? , & Dr. Atia Sharmin Bonna ¥ disease. Due to the fact that asymptomatic individuals seldom seek medical attention, the real prevalence of CAD has been grossly underestimated since childhood. 4 Heart failure is a risk factor even in those without coronary artery disease. The exact process by which obesity causes heart failure without coronary artery disease is uncertain, although two major ideas exist. 5 Firstly, fat people have more blood in their bodies, which makes the heart work harder and can lead to heart failure in the long run. ventricular hypertrophy is a condition in which the heart's muscle size increases as it works harder. Obesity has also been related to sleep apnea, which can lead to respiratory problems and high blood pressure in the long term. 6 The major objective of this study is to examine the obesity impact and its link to coronary artery disease (CAD).
2. II.
3. Objective a) General objective
? To evaluate the obesity effect and its relationship to CAD.
4. b) Specific objective
? To detect risk factor of CAD. that are associated with obesity. Cardiovascular disease is more common in those who are obese in the abdominal area (central obesity or "visceral obesity"). [1][2][3] It has been estimated that between 12 and 16 percent of Indians are affected with coronary artery disease (CAD). Five-fifths (52 percent) of all CVD-related fatalities occur among persons under the age of 50, and about a quarter of all acute myocardial infarctions (MI) occur in those under the age of 40 in India as well 4 Patients who seek medical attention owing to symptomatic sickness may represent the "tip of the iceberg" when combining visible and subclinical diabetes and smoking were all gathered using a WHO-STEPS modified methodology.
5. d) Statistical Analysis
? A pre-formatted data sheet was used to capture all data, and the data was then analyzed using applicable statistical techniques using Microsoft Windows software version 20. Simple percentages were used to assess the prevalence of hypertension. t-tests and chi-square tests were used to determine the significance of the results. At a threshold of 95 percent (p =0.05), all statistical tests were judged significant.
IV.
6. Result
In table-1 shows age distribution of the patients where for both male and female, most of the patients belongs to (41-50) age group, 57%. The following figure is given below in detail: In figure-2 shows gender distribution of the patients. Where among 150 patents male patients were 30% higher than female. The following figure is given below in detail: V.
7. Discussion
This cross-sectional study was designed to determine the incidence of cardiac disease in obese Bangladeshi adults who were overweight or obese. As a major risk factor for cardiovascular disease (CVD) or heart disease, obesity must be addressed.
All research subjects had their blood pressure measured, and we found that the blood pressure of the obese group was statistically significantly greater than that of the normal weight group. Obesity was more prevalent in this study than in the previous one, as we found out during our research process. 6 Overweight and obesity are significant problems in Bangladesh and other developing countries.
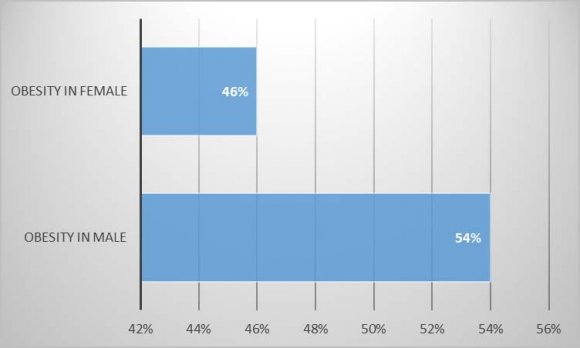
The prevalence of obesity is expected to be higher in older populations than in younger populations, such as Bangladesh and India, although studies have shown that hypertension is common in developing nations 7,8. As people age, they are more likely to become fat, which is in line with previous studies. 9 According to this survey, 54 percent of males and 46 percent of females are obese. There was no statistically significant difference between males and females despite the greater incidence rate. People with heart disease are more likely to have obesity-related hypertension. Another study done in India's rural areas came to the same conclusion. When we looked at patients with positive cardiac illness, we found a significant prevalence of obesity.
Our research revealed that systolic and diastolic hypertension affected 24 and 28 percent of the 100 individuals, respectively. On the other hand, one research revealed that individuals with MI had a larger impact from elevated systolic blood pressure than from elevated diastolic blood pressure Endothelial damage induced by high systolic blood pressure might be the reason, leading to increased atherosclerosis. It has long been recognized that high levels of triglycerides, total cholesterol, and LDL cholesterol in the blood are associated with cardiovascular disease.
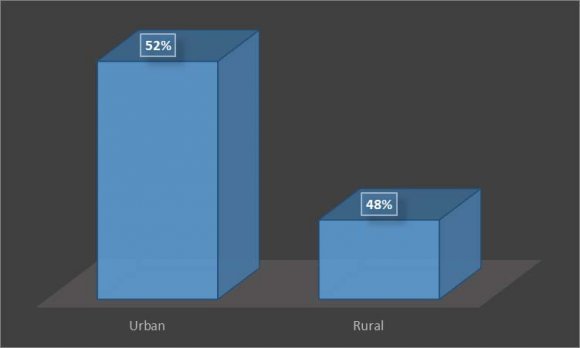
Similarly, obesity and salt consumption were linked in another research along with age, body mass index (BMI), physical inactivity (including smoking), and a family history of stroke/CVD. 5 The growing salinization of freshwater puts more than 35 million people in coastal Bangladesh at danger; increased salinity in drinking water has been related to higher blood pressure among youthful coastal populations. Since the majority of patients were from rural regions, they may not be aware of the hazards of drinking water salinity, which is why we found a high correlation with this report during the research.
Many individuals assume that cooking renders the salt safe. Weight gain, a recognized risk factor for coronary atherosclerosis (CAD), is considered to be made worse with an excessive salt intake. 10 VI.
8. Conclusion
We can draw the conclusion that obese individuals in Bangladesh have a higher risk of developing heart disease than other patients. In order to establish the prevalence of obesity in heart illness, more study is needed.

| Age group | % |
| 21-30 | 6% |
| 31-40 | 8% |
| 41-50 | 57% |
| 51-60 | 20 |
| 61-70 | 9% |
| Risk Factors | (n = 150) % |
| Smoking | 52% |
| Hypertension | 63.5% |
| Dyslipidaemia | 74% |
| Obesity | 79% |
| DM | 30% |
| Family history | 26% |
| Sedentary life style | 19% |
| Figure-5: |
| Year 2021 | |||
| 34 | |||
| Volume XXI Issue VI Version I | |||
| D D D D ) | |||
| ( | |||
| Medical Research | |||
| Global Journal of | CORRELATION OF OBESITY WITH FAMILY HISTORY SMOKING | R-VALUE -.229 -.124 | P-VALUE <0.01 <0.01 |
| INCOME | -.130 | <0.01 | |
| OCCUPATION | .008 | >0.05 | |
| PHYSICAL ACTIVITY | -.142 | <0.01 | |
| HYPERTENSION | -.289 | <0.01 | |
| BMI | .276 | <0.01 | |
| GENDER | -.022 | >0.05 | |
| AGE | -.285 | <0.01 | |
| HEART DISEASES | -.286 | <0.01 |