1. Introduction
he disease atherosclerosis has great relevance today. Atherosclerosis is a distinctive form of arterioscleorosis known from ancient times. The terms 'athere' (meaning-porridge) and sclerotic (hardening or fibrosis) derived from Greek terminology, do not represent the complete morphology of disease. Despite our familiarity with this disease, some of its fundamental characteristics remain poorly recognized and understood. The cause and pathogenesis of atherosclerosis remains subject of lively speculation and controversy. 1 Atherosclerosis is a pathological entity and a multifactoid disease of large and medium sized arteries, characterized by plaque like intimal deposits which contain neutral fats, cholesterol, lipophages, blood elements, at times, other evidence of hemorrhage and calcium deposits. Complications of which are disastrous -ischaemic heart disease, cerebral stroke, peripheral gangrene and so on. It is a pandemic, percentage incidence of morbidity varies from country to country. It is a modern epidemic in U.S.A., Europe, Canada, New Zealand and Australia. 2 Among the diseases in the western world, atherosclerosis is overwhelmingly the prime disorder leading to death and serious morbidity. Despite recent reduction in mortality of coronary heart diseases (CHD) about 50% of all deaths in US are still attributable to atherosclerosis related diseases. 1 The developing countries such as India, Singapore, Malaysia and Sri Lanka are catching up and registering a steady increase in the mortality rates due to atherosclerotic heart diseases. 3 In India coronary heart disease accounts for 10-15% of all cardiovascular diseases. 4 The exact global incidence of atherosclerosis is impossible to calculate because it can exist without producing any symptoms or signs. These asymptomatic cases can be diagnosed only if an autopsy is done, in all cases of death due to any cause. However, the magnitude of the problem can be assessed by looking at the mortality rates in different countries due to atherosclerotic heart disease. In a survey conducted in males in the 45 to 54 years age group, 5 the mortality rates due to atherosclerotic heart disease in different countries are lowest in Japan (8%) and highest in Finland (41%). In U.K., U.S.A., and Canada the average mortality rate is 36%. The disease is increasing in countries undergoing industrialization. 6 Unfortunately, in India there are no statistics giving the national incidence of this disorder. 3 However, Padmavathi and associates, 7 gave the average incidence of atherosclerotic heart disease in seven different states during 1958-59 as 0.51% per 1,000 population. In another study conducted at All India Institute of Medical sciences, New Delhi, with the help of autopsy studies and taking atherogenic index as an indicator, the incidence of coronary heart disease is given as 35.5% in males and in females as 14%.
Although global incidence, a wide range of variation in the prevalence and severity of atherosclerosis has been shown to exist in different geographic population. Against this background the present study has been taken in order to determine the severity and distribution of coronary atherosclerosis in the selected autopsies of the deaths occurring in general population Karnataka state, which has good representation of all social classes. 5 II.
2. Methodology a) Materials And Methods
The material for the present study included 50 (fifty) heart specimens obtained from medico legal autopsies performed in the Department of Forensic Medicine, Basaveshwara Medical College and Hospital, Chitradurga and other heart specimens received at the Department of Pathology, Basaveshwara Medical College and Hospital, Chitradurga, sent for histopathological examination to define any suspected cardiovascular pathology. Hearts were obtained by standard procedures from all autopsies.
The age, sex and relevant information including age, sex, socio-economic status, dietary habits of the deceased were obtained from the informant accompanying the deceased.
The methods used for the analysis of the material was as per the procedure recommended by 1. White, Edward and Dry (1950). 2. Gore and Tejada (1957). All autopsies were carried out within four to twenty four hours after death. 10,11,12 All the specimens of right and left coronary arteries blocks were taken at a particular fixed distance at from 1.5 cm and 3 cm from the Ostia, also From the circumflex branch of the left coronary artery, bits were taken at the same distance form the point of branching of the left coronary artery into anterior descending and circumflex branches. Additional bits of tissue were taken from other regions of the vessels which showed stenosis. This stenosis is graded based on the luminal narrowing of the coronaries when examined by hand lens and is graded from grade 0 (no narrowing / normal) to grade IV (complete obliteration). Grade -0 : Normal Grade -I : 1-25% stenosis Grade -II : 26-50% stenosis Grade -II : 51-75% stenosis Grade -IV : 76-100% stenosis The bits of the tissue were fixed in 10% formalin and embedded in paraffin. Sections for histological study were taken from the paraffin blocks and stained with haematoxylin and eosin. Special stains were also done whenever indicated, namely Verhoeff and Van-Gieson's for demonstration of elastic tissues, smooth muscle and collagen, and Alcain blue for the demonstration of mucopolysaccharide ground substance. All histological sections were studied for microscopic evidence of atherosclerotic lesions.
3. III. Results
The coronary arteries of fifty specimens of heart were examined in the department of Pathology, Basaveshwara Medical College and Hospital, Chitradurga, observations made from the study are as follows:
The youngest subject was 19 years and the oldest was a male of 80 year age, forming a age range of 19-80 years. The majority of the cases were from 3 rd to 4 th Of the 50 cases studied 33 cases showed coronary atherosclerosis. This table shows that coronary atherosclerosis will increase with age and it also shows that males are more affected i.e., 24 cases (72.72%) and females are affected in 9 cases (27.27%). The coronary atherosclerosis was much common in males but after 5 th Graph 3 : Coronary Atherosclerosis decade it takes the same course in both male and female.
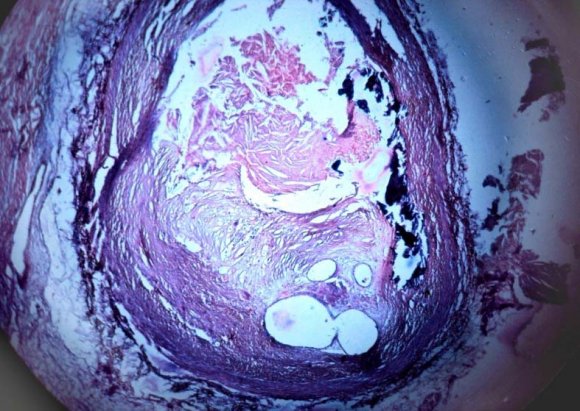
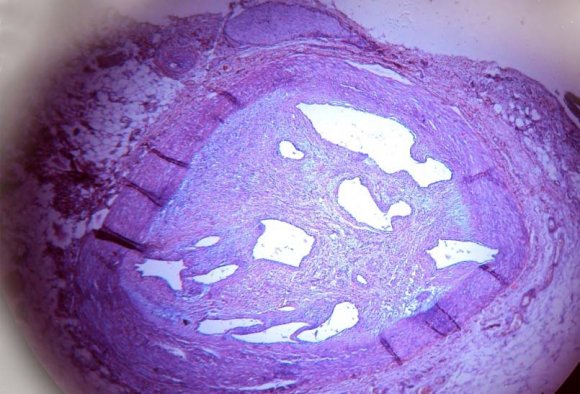
Of the 50 heart specimens studied 33 showed coronary atherosclerosis with various histological changes such as fibroblastic activity, mucopolysaccharide deposition, degeneration of internal elastic lamina, accumulation of lipid cholesterol crystals, hyalinization, calcification and hemorrhage. Salient features of atherosclerotic lesions i.
Fatty streaks. ii.
Fibrous plaques. iii.
Atheroma. Histological, examination of representative plaques in the second and third decades showed the presence of fat with little or no cellular reaction. In the 4 th and 5 th decades, there was generally a fibrous tissue reaction to the presence of fat. By the 5 th decade, the fibrous reaction had become more pronounced and was associated with degenerative changes.
4. Discussion
The autopsy study provides a means of understanding the basic process which sets a stage for clinically significant atherosclerotic cardiovascular disease. There is no valid method of sampling of living population. It was, therefore, considered that deaths suspected due to cardiovascular pathology, probably provide the best sample of the living population for studying atherosclerosis. Many epidemiological studies have brought to light a number of factors that are of indisputable importance in the development of atherosclerosis. In the present study the cases from the first decade were not included as the disease started in the 2 nd decade, as stated by Gore et al (1960). 9 Wig 13 In the 2 and associates observed that atherosclerosis started appearing in teen age itself. nd decade, the incidence of atherosclerosis was 50% in the present study which was higher compared to Wig 13 and Associates Study (38%) and Bhargava's 16 Study (10%). This may be due to small sample survey. Results of third decade were almost similar to the Wig and Associates, 40% incidence in the Bhargava's Study which was lesser when compared to present study (66%). The increase of incidence in our study may be due to change of life style of people in recent decades.
After fifth decade almost all the cases in the present study showed the evidence of atherosclerosis. The present study was almost comparable to the above studies in the remaining decades.
V.
5. Conclusion
The present study concludes that coronary artery atherosclerosis is common in majority of cases. Atherosclerosis is a complex and multifactorial disease. Age has a dominant influence. Males are affected more than females. Smoking and alcoholism can accelerate the development of atherosclerotic lesions, though they are not atherogenic on their own.
All the observation in the present study showed that the incidence of atherosclerosis in the developing countries (like India) is same as developed countries. There is need of life style change in general public as well as cardiologists and treating physicians to think of early treatment, to avoid untoward complications.



| Habit of Smoking | No. of cases | Positive cases No. of cases Percentage | |
| Smokers | 24 | 19 | 79.16 |
| Non-smokers | 26 | 14 | 53.84 |
| Total | 50 | 33 | - |
| The above table showed higher incidence in | |||
| smokers (79.16%). When compared to non-smokers | |||
| (53.84%). | |||
| Graph 1: Smoking and Atherosclerosis | |||
| 2 : Alcoholism and Atherosclerosis | |||
| Alcoholism and habit | No. of cases | Positive cases No. of cases Percentage | |
| Alcoholics | 23 | 18 | 78.26 |
| Non-alcoholics | 27 | 15 | 55.55 |
| Total | 50 | 33 | - |
| Incidence of atherosclerosis was greater in | |||
| alcoholics (78.26%) than in non-alcoholics (55.55%). | |||
| Age group | Sex | Total No. of cases | No. of cases positive | Total positive | Percentage |
| 11-20 | Male Female | 2 2 | 2 0 | 2/4 | 50 |
| 21-30 | Male Female | 6 2 | 4 1 | 5/8 | 62.5 |
| 31-40 | Male Female | 12 5 | 7 3 | 10/17 | 64.7 |
| 41-50 | Male Female | 8 4 | 5 3 | 8/12 | 66.66 |
| 51-60 | Male Female | 5 1 | 4 1 | 5/6 | 83.33 |
| 61-70 | Male Female | 1 1 | 1 1 | 2/2 | 100 |
| 70 and above | Male Female | 1 0 | 1 0 | 1/1 | 100 |
| 50 | 33 | 33 | 66 |
| Study | Place | Percentage | ||
| 1. | Wig and associates (1962) | 13 | North India | 64 |
| 2. | Enos et al., (1953) 14 | Korea | 77.3 | |
| 3. | Subramaniam R. et al., (1964) 15 | Madras | 62 | |
| 4. | Bhargava and Bhargavan (1975) 16 | North Karnataka | 69.9 | |
| 5. | Shirani J et al., (1995) 17 | USA | 65 | |
| 6. | Strong J.P. et al., (1999) 18 | USA | 60-80 | |
| 7. | McGill et al., (2000) 19 | USA | 58 | |
| 8. | Present Study | karnataka | 66 | |
| comparison with the present study | ||
| Study | Age range | |
| 1. | Wig and Associates, (1962) 13 | 0-80 |
| 2. | Enos et al., (1953) 14 | 18-48 |
| 3. | Subramaniam R. et al., (1964) 15 | 2.5-94 |
| 4. | Bhargavan and Bhargava, (1975) 16 | 0-90 |
| 5. | Shirani J. et al., (1995) 17 | 71-80 |
| 6. | Strong J.P. et al., (1999) 18 | 15-36 |
| 7. | McGill et al., (2000) 19 | 15-34 |
| 8. | Present study | 19-80 |
| Decade | Wig and Associates (1962) 13 No. with lesions % | Bhargava and Bhargava 16 (1975) No. with lesions % | Present study No. with lesions % | ||||
| < 1 year | - | - | 0/13 | 0 | 0 | 0 | |
| 1 st | Decade | 2/18 | 11 | 2/20 | 10 | - | - |
| 2 nd | Decade | 7/18 | 38 | 2/21 | 10 | 2/4 | 50 |
| 3 rd | Decade | 24/38 | 63 | 12/30 | 40 | 5/8 | 62.5 |
| 4 th | Decade | 23/24 | 95 | 21/25 | 84 | 10/17 | 64.7 |
| 5 th | Decade | 23/25 | 92 | 17/21 | 80 | 8/12 | 66.66 |
| 6 th | Decade | 19/19 | 100 | 10.12 | 83 | 5/6 | 83.33 |
| 7 th | Decade | 8/9 | 88 | 3/3 | 100 | 2/2 | 100 |
| 8 th | Decade | - | - | 1/1 | 100 | 1/1 | 100 |