1. Introduction
nthropometric data collection is a tool widely used today in design and development of a product. The use of the Anthropometric data during the design stage assists in the optimum use of the product by target population for intended application. National institute for occupational safety and health (NIOSH) conducted an anthropometric study of the facial measurements (NIOSH 2007). The safety of the population using the respirators is addressed by the NIOSH and it is the responsibility of NIOSH to ensure that quality of the respirators is maintained and it fits to the target population. Hence NIOSH conducted an anthropometric survey of sample population depicting the diverse US respirator users. The manufactures also followed the guidelines given by NIOSH. An overview of the airway geometry is needed by many for the purpose of studying the airflow dynamics involved. Figure 1 shows a numerical study of the spray particle deposition in the human nasal cavity and the geometry used. The volume of intake air first comes in contact with the anterior portion of the nasal cavity and oral cavity (during oronasal breathing). These two regions get first affected by the fluid intake. The geometry of the nasal cross section is very complex and asymmetric in nature. These dimensions are measured using scanning and imaging methods for measuring the cross-section in the middle region consisting of the turbinate's and the posterior region connecting to the Nasopharynx. The Anterior portion can be measured using the available device patented (US6659963) shown in Figure 2. The Oral cavity when compared to the nasal cavity is convenient to measure until the throat region.
Data collections for the anthropometric measurements are usually related to the measurements externally and not internally due to the complexity of the human body. The anthropometric data measured for the external body comprise of number of subjects up to 4000 in number and more. The morphometric studies conducted for the internal body consisted of approximately 100 subjects at the maximum. The reason here is that the internal studies need sophisticated equipments like CT or MRI scans etc whereas the external anthropometric measurements need basic measuring instruments like callipers and measuring tape. The usage of the imaging devices is a complicated procedure and needs to be done by medical providers. The use of these equipments could be complicated, time consuming and cost will be staggering for a large population sample size. The same when performed by the use of the measuring devices for external anthropometric measurements will not be as expensive and complicated as for example the use of imaging devices.
The anthropometric data related to the volume of the nasal and oral cavity has been measured using imaging devices using small sample size. A measuring technique is proposed here in to measure the dimensions of the nasal and oral cavity with help of measuring instrument. The instrument could be used for measuring the inside dimensions of the nasal and oral cavity. This process of collecting anthropometric data for the human nasal (anterior portion) and the oral cavity (mouth portion) will provide the much needed data to help with the treatment of injuries, design of the respirator systems and other respiratory devices.
2. Overview of Current Methodology
A number of approaches are in the literature that study the characteristics related to heat and mass transfer along the HRT, deposition of particles, drug therapy applications and injury analysis. These studies do involve taking measurements of the various portions of the upper (nasal and oral) respiratory tract. The Human body does show a high degree of variation between different Human races around the world. The Anthropometric data collection for the human respiratory tract can be identified in two different categories, first in which the measurements for the internal portion of the HRT are taken into consideration for the analysis of the process of heat transfer characteristics, burn injury and or aerosol deposition taking place and in the second category the facial dimensions are noted down to assist fitting of the respirator device on the human face for fullface piece respirators or half-face piece respirators. The categories when analyzed are from a completely different point of view but when the functionality is taken into account; the facial characteristics and the inlet portion of the nasal and oral cavity are directly related to the effective functioning of the human being using the respirator device. The current methodology of gathering the anthropometric data are limited in both the cases. For the category 1 the inlet dimensions of the HRT are identified using the process of CT scan, MRI and Acoustic Rhinomanometry which is a costly process and can be performed on a limited number of subjects. The use of scale, callipers and tape for the category 2 type has been extensively used. This method has been performed on a number of subjects but it has its limitations as it can measure only the facial dimensions from outside.
3. III.
4. Literature Review
A geometric model was developed for the human nasal cavity using CT scan images (Liu et al. 2009). This was done in collaboration with a hospital's Otolaryngology department and a subject size of 30 was used in the study. The model created was then compared with that available in the literature and a satisfactory model for the nasal cavity was obtained. The CT scan available was first converted into 2D coronal cross-sectional slices and with this as a reference a new 3D geometry was developed. The model completely focuses on the nasal cavity until the posterior region just above the nasopharynx. The fact that the deposition along the respiratory tract is influenced by the three major factors: physical, physiological and morphological is evident (Cheng et al. 1996). To study the aerosol deposition in the human nasal and oral cavity the authors here measured in vivo nasal cavity dimensions using both MRI and AR. A 3D model was reconstructed for oral cavity and the throat model using casting procedures (Robinson et al. 2009). The authors here implemented the casting method instead of the MRI citing that accurate geometry is not obtained due to the movement of the vocal folds during breathing. Grgic et al. studied the aerosol deposition and flow measurements using a human mouth and throat replica (Grgic et al. 2004). The mouth piece angle and dimension were selected from that available in the literature for straight tubes. The extrathoracic model developed here was generated using the information available from CT scans, MRI Scans and observation of subjects during breathing. The model generated consisted of the mouth, oropharynx, larynx and the trachea. Furthermore a study the inter-subject and intrasubject in realistic mouth-throat geometries including mouth, oropharynx, larynx and trachea was also concluded (Grgic et al. 2004). The models used for these purposes were obtained using MRI scans of seven geometries. The acoustic reflection (AR) was used to study the nasal cavity geometry and dimensions (Hilberg et al. J create a good fit of the respirators for the entire US respirator users. The anthropometric survey here consisted of a sample size of 4026 subjects for a total of 18 facial and head dimensions manually. The Anthropometric measurements specified above were from externally/ facial features, measuring the internal dimensions in the nasal and oral cavities can also be considered.
IV.
5. Methodology
The Nasal cavity geometry follows a highly complex and asymmetric shape after a length of about 30 mm from the nasal inlet. The process of capturing the characteristics of this region is challenging task. The first 30 mm length of the Nasal cavity is the anterior portion which first comes in contact with the flow during inlet as shown in Figure 3. Figure 3 shows the imported geometry with mesh constructed for the simulation run. The mesh generation process here is determined by the value of the Reynolds number and the Reynolds number used here is 4130 (See Appendix 1) based on the diameter of the trachea and k-? turbulence model is used for turbulent flow of low Reynolds number.
During a hazardous situation if hot air is inhaled then degree of burn injury suffered could be very high. The dimensions can be measured if an appropriate measuring device is designed for this particular task. The procedure for using this type of tool which penetrates into anterior portion of the nasal cavity must be performed under medical supervision. Figure 4 shows a measuring device (patent number US6659963) designed to measure the cavity in the anterior portion of the nasal cavity in between the inlet and the nasal turbinate's.
The device consists of three different tubes of varying length and diameter. The tube E has a calibrated scale shown in red colour. The tube B and D are connected by a wire mesh A. The wire mesh A expands or contracts when the tube D is moved in the horizontal direction i.e. inwards or outwards. The outer tube C acts as support for the two sliding tubes within. The portion of the tool that penetrates into anterior portion of the nasal cavity is highlighted in Figure 2. When the portion is inserted into the cavity and the tube is moved horizontally until the wire mesh obstructs the sliding mechanism, the data can be noted down from the calibrated scale. Figure 3 shows the pictorial of the existing measuring device.
The dimensions of the Oral cavity can also be measured internally. A measuring instrument similar to a calliper can be used to measure distance in 2 or 4 or 8 directions. This procedure might not need the degree of medical supervision as in the case of the Nasal cavity measurement but it is advisable to have a guidance of a medical practitioner. Figure 4 shows an arrangement of the instrument designed to measure the oral cavity dimensions. The end portion A is inserted into the mouth while the handle D is manipulated. The ends "A" are placed against the wall of the oral cavity and the displacement of ends "A" is measured from the calibrated scale C. The two handles B pivot about the point F to place the two ends "A" against the wall tissue inside the oral cavity. Point E is free to move along the curvature of the handles "B".
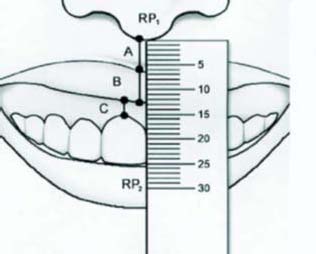
The instrument shown in the Figure 5 could be used to measure the dimensions of the oral cavity as identified in Robinson et al. ( 2009) as a guideline. The inlet of the oral cavity is the widest and follows a tapering cross-section has it advances horizontally towards the Oropharynx. The outermost width being 30.9 mm and approximately 20 mm in width when measured 54 mm deep within the oral cavity as shown in Figure 6. Figure 7 shows the instrument with measurements from Robinson et al. ( 2009) used as a reference for design such that the instrument is capable of measuring the widest distance close to the oral cavity inlet and the lowest width which is at a distance of 54 mm from the opening.
V.
6. Discussion
The methodologies used for the purposes of the data collection can be summarized as the use of MRI, CT Scans, AR and use of Casting. This type of data collection usually is used on a small number of subjects. The limiting constraints include cost and subject availability due to the nature of procedures. A simple approach to measure these anthropometric data may lack the sophistication of the scanning and imaging devices like CT scan, MRI and AR but will provide the ability to measure large number subjects leading to more statistically usable data. The usages of the MRI, CT scan and AR have disadvantages of being unsafe from ionizing radiation or high costs of using the equipment and use.
The advantages of using this process of identifying the internal nasal and cavity dimensions can be attributed to the fact that this process can be applied to a large sample group. The cost involved with the use of the scanning and imaging devices will also be eliminated by this process. Exposure to the scanning and imaging devices also has a possibility of causing injury to the human body which can be eliminated by the use of these tools. The drawback of this method would be that the measuring needs to be done by the medical providers as the measuring device is inserted into the human body and not similar to the case in measuring the external anthropometric data. The Anthropometric data obtained here will have the measurements of the nasal cavity at a maximum of 50 mm deep and 54 mm for oral cavity whereas the scanning and imaging devices will assist in measuring within the human body.
A feasible method of measuring the dimensions of the Nasal and Oral cavity needs to be developed. A J measuring instrument similar to a calliper can be used to measure distance and or volume within the cavity. The process of measuring the anthropometric data here first starts with defining the landmarks in the human body, for example the tip of the nasal or oral inlet being one of the landmarks in the data collection process followed by the data analysis.
VI.
7. Conclusion
In this study, an approach of measuring the nasal and oral cavity dimensions is outlined for research purposes. Anthropometric data are needed for the design and development of certain respiratory devices and instruments such as safety masks and goggles, respiratory masks, inhalators, etc. and treatment of the respiratory tract after injury. Various three dimensional heat transfer model of heated airflow through the upper human respiratory tract consisting of nasal, oral, trachea and the first two generations of bronchi are developed based on anthropometric dimensions for the various populations. Using computational fluid dynamics simulation software mesh diagrams of oral and nasal cavities considering various breathing / flow configurations are simulated based on these models. Other research uses include the study of the heat and mass transfer, aerosol deposition and flow characteristics in the upper human respiratory tract using computational fluid mechanics simulation requires access to a two dimensional or three dimensional model for the human respiratory tract.
Depicting an exact model is a complex task since it involves the prolonged use of imaging devices on the human body. Hence a three dimensional geometric representation of the human upper respiratory tract is developed using anthropometric data collected consisting of nasal cavity, oral cavity, nasopharynx, pharynx, oropharynx, trachea and first two generations of the bronchi. The methodology would measure the characteristic dimension of the human nasal and oral cavity at the inlet/outlet points which are classified as internal measurements. The respiratory tract is modeled circular in cross-section and varying diameter for various portions as identified and characterized by the anthropometric data. Based on the dimensions identified, a simplified 3D model representing the human upper respiratory tract is generated.