1. Introduction
he motorcycle has evolved over the years as a means of transportation. In developing countries it serves as a mode of commercial transportation ferrying passengers from place to place. Their operators are mainly youths who are untrained and sometimes drive under the influence of alcohol. Safety and security concerns have been raised by stakeholders and this has led to the total ban of motorcycles as mode of transportations in some major Nigerian cities like Lagos and Calabar. The incidence of motorcycle accident i cities like Lagos and calabar is as high as 27% 1,2. In Sokoto metropolis, motorcycle accidents constituted 40% of road traffic accidents in 2009 3.
In the United States available statistics indicates that motorcyclist are 35 times more likely to experience a deadly accident on the road than those in passenger car and 11% of all road accidents involves motorcycles 4. The vulnerability of users of motorcycle as means of commercial transportation makes them a target audience in injury prevention strategies 5, 6, 7.
The pattern of injuries resulting from motorcycle accidents is varied with musculoskeletal and head injuries being the most common. Sokoto is a cosmopolitan city in Northwestern Nigeria and has a population of 427,760 as of the 2006 census. Sokoto lacks a public transport system and it is easier to commute by the aid of a motorcycle as is the case in some Nigerian cities. Patronage of commercial motorcyclist cuts across social economic status as some do use them to navigate the poor road network and sometimes to beat traffic. Stakeholders in road safety have raised concerns about the safety of this mode of transportation. Efforts at enforcing safety measures through the use of crash helmets have been largely unsuccessful. It is against this background we sought to determine the injury severity in victims of motorcycle accidents in Sokoto, North Western Nigeria.
2. II.
3. Methodology
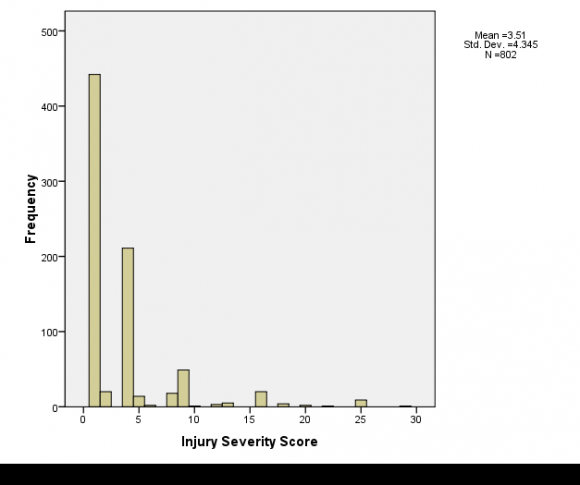
This was a prospective descriptive study of victims of motorcycle accidents carried at the trauma Centre of a tertiary hospital in Sokoto, North-West, Nigeria over a period of one year from January 2012 to December 2012. The trauma Centre caters for patient from Sokoto metropolis, neighboring cities and states. Trauma records of victims of motorcycle accidents (MCA) were recorded in a proforma that included the age and sex, class of victim in terms of rider, passenger or pedestrians. Other information gathered was the nature of collision motorcycle-motorcycle collision (MMC), motorcycle-car collision, lone motorcycle accidents (LMA) and motorcycle-pedestrians' collision. The use of helmets amongst rider and passenger, the injury severity score and outcome were also recorded. The injury severity score (ISS) system is a process by to a single number. It is an anatomical scoring system and can be determine by the attending casualty doctor. Each injury was assigned an abbreviated injury scale (AIS) in the six body region of Head and Neck, Face, Chest, Abdomen, Extremity and External. AIS range from 1 to 5 depending on the severity of injury. Minor injuries were assign 1, moderate 2 and severe 5. The 3 most severely injured body regions have their scores squared and added together to produce the ISS. The least ISS is 1 and the highest is 75. Score reflective of injury severity include 1 to 9 as Minor, 10 to 15 as Moderate, 16 to 24 as Moderate to Severe and 25 an above as Severe to critical.
Statistical analysis was done with SPSS 17 and results presented as graphs.
4. III.
5. Results
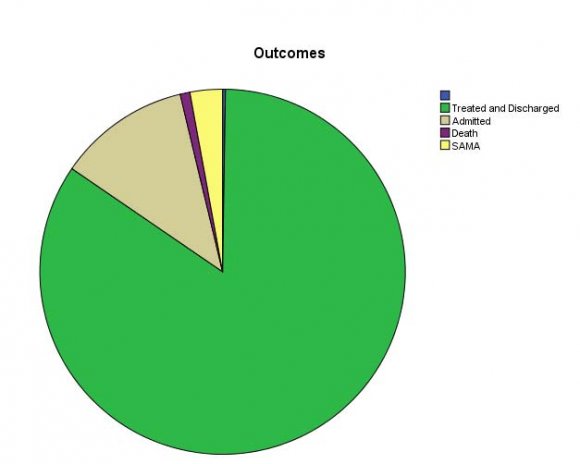
A total of 803 victims of motorcycle accidents were seen over the 12 months period with majority of victims in the age range of 21-30 years representing 44.3% follow by those within the age range of 11-20 and 31-40 with 21% and 15% respectively as shown in figure 1. Time of arrival in hospital from the accident site showed that 79.8% of victims arrived at the hospital in less than 2 hours while 20.2% arrived between 2 to 6 hours. The male to female ratio is 7:1. Most of the accidents occurred in the months of October 13.8%, May 13.2%, June 11.7% and April 11.0 % as shown in figure 2. Fifty-five per cent of victims were the riders while passengers and pedestrian constituted 34.8% and 9.8%. The nature of accident was such that 43.6% were victims of motorcycle versus motorcycle collision while 24.2% were victims of lone motorcycle accidents. Lone motorcycle collisions are crashes with stationary objects or where there is loss of control. Victims from motorcycle and car collision were 21.9 %. Motorcycle-pedestrian collision resulted in 10.3% of victims. None of the riders and passenger used protective helmet. Eighty-one per cent of victims had injury severity score ISS of 4 and below while the highest ISS of 29 was seen in one victim as shown in figure 3. Eighty four per cent of victims were treated and discharge while nine victims died. Twelve per cent of victims were admitted for further management while 3% signed and left against medical advice.
IV.
6. Discussion
Majority of our patients were below 40 years with a peak at 21-30 years and this was similar to findings in North Central Nigeria 8. These are the productive age group in the society: and with increasing unemployment the business of commercial motor transportation becomes a ready alternative. There was a preponderance of male victims as is in some other studies 1, 5, 8.
The female victims are either passengers or pedestrian as none was a rider. The practice of commercial motorcycle transportation is usually the exclusive preserve of the men. Sociocultural and religious considerations are major determinants of economic adventures in this part of the world.
Majority of the victims arrived at the Centre within 2 hours and delays usually results from the absence of ambulance service and lack of a prehospital emergency preparedness plan 9. It is also not unusual to have delays from arguments among riders and drivers of commercial vehicles trying to establish who is at fault rather than see to the rescue of affected victims to hospital.
Our study noted that the highest numbers of patients were seen at the beginning and in the peak of the dry season. Rain and poor weather conditions affect outdoor activities and for motor cycle transport business, this may be far reaching. This could explain the increased numbers seen during the dry season.
Majority of the victims were the riders while most victims were from a motorcycle to motorcycle collision. This goes to show the level of training and recklessness of some of these riders. The business of commercial motorcycle transportation is an all comers affair. Riders are not licensed and they do not have regards for road signs. In a study in Ilorin, North central, Nigeria, motorcycle-vehicle collision produced the largest amount of victims 10. The number of victims was almost twice as high in motorcycle-motorcycle collision as in motorcycle-vehicle collision in our study. This may be an indication that the numbers of motorcycle plying the roads are high. This may also be an indication of the level of impatience associated with some of these riders. Reasons adduced for the high number of motorcycles on our roads include cheaper cost of acquisition compared to cars, increasing fuel cost and sometimes these motorcycles are given out to youths as gratifications by politicians. Other reasons are that most of our cities lack good road network and public transport system and for the inpatient individuals the motorcycles serves as a means of navigating traffic 10, 11, 12.
Another worrisome trend is the number of victims from lone motorcycle accidents. From the mechanism described earlier it shows that some of these riders are either under the influence of drugs or they are too reckless or they are not trained. Studies in Zaria, a city about 450 km South-east from our study city indicated a high prevalence (59.5%) of use of psychoactive drugs amongst motorcycle riders involved road traffic accidents13.
The use of helmet has been a difficult safety measure to enforce in most Nigerian cities especially in the northern part where cultural and religious reasons have been adduced for their non-compliance. While the as a result of legislation, that cannot be said of developing countries. A study in Thailand showed a high number of helmet use in riders of about 60% while only 28% of passengers reported they always wore helmet 14. Reports from some Nigerian cities show the near absence of helmet use either by the riders or passengers 10, 15.
Majority of the victims had injury severity that was termed minor and this includes bruises and lacerations. About half of the victims were from a motorcycle-motorcycle collision and this could explain the severity of the injuries sustained. MMC results in low energy collision while injuries sustained from a motorcycle-car collision or from a lone crash or motorcycle-pedestrian collision are likely to be more severe because of the seemly high energy involved. In all the events, the rider and passenger are vulnerable in the crash because of their lack of protection. It should be noted cases of fatality from motorcycle accidents occurring at the scene of the accident were not included in the study, hence the injury severity that appears to be low only tells of those that were rescued to hospital.
Traumatic brain injuries (TBI) and thoracic trauma as well as abdominal injuries are common fatal injuries sustained in motorcycle accidents12, 15, 16. While these major traumatic events can be handled in developed countries with established pre-hospital care, thus reducing mortality to the least, the same cannot be said of poor and developing countries with absent prehospital care. Deaths from secondary brain injury and hemorrhage occur from delays in accessing health care and inappropriate triage 11, 16.
The injury severity score system was used to assess the degree of injury sustained, the limitation of this anatomic based system is that it does not reflect the seriousness of the injuries. It was however chosen because of the simplicity of scoring as various officers were involved.
Mortality was quite low and this may be a reflection of the degree of severity and the fact that a dedicated Centre is involved in the care of traumatic surgical emergencies.
V.
7. Conclusion
The study found out that injury severity amongst victim of motorcycle accident can be categorize as minor, the large number of victims however shows that commercial motorcycle transportation is inevitable in developing society like ours. Regulation of motorcycle riders in terms of licensing, numbers, education and enforcement of use of helmet can reduce the number of motorcycle accidents.