1. Introduction
he coeliac trunk is the first ventral branch of the abdominal aorta and it supplies the supracolic organsThe Coeliac trunk arises at the level of T12/L1 vertebral bodies just below the Aortic hiatus. It is 1.5-2 cms long and passes almost horizontally forwards and slightly to the right above the pancreas. (1).
According to standard anatomical textbook descriptions, the coeliac trunk and its branches supplies the gastrointestinal tract from the lower 1/3 rd of the esophagus to middle of 2 nd part of the duodenum and all derived adenexae (liver, biliary tree, spleen, pancreas, greater and lesser omentum).
When there is one vascular variation, there is a high chance of multiple variations. T he arterial architecture is important in a patient undergoing surgery in this area or it may lead to a risk of an error in committing lethal complications.Variations of these arteries and their relationship to the surrounding structures are of particular importance from a surgical perspective.Incidence and variation in the branches of the CT requires specialized preoperative diagnostic knowledge.
An anatomical variation of the coeliac trunk and hepatic arteries hasconsiderable importance in liver transplants, hepatobilary manipulations, laparoscopic abdominal surgery, radiological abdominal interventions and penetrating injuries to the abdomen. The aim of the present study was to highlight the additional branches arising from the CT and discuss their topography, which may be important for surgeons operating in upper abdominal regions.Presence of additional arteries may provide collateral circulation which is essential during transplant surgeries. We looked at these vascular systems in routine cadavericdissections. .
2. II.
3. Materials and Methods and Observations
The branching patterns of the Coeliac trunk was done on 40 embalmed cadavers (34 males and6 females) which were used during routine dissection by undergraduate I MBBS students from the Department of Anatomy for a period of 3 years .The abdomen region was dissected out carefully for Coeliac trunk and their branches by retracting the stomach and the small intestine. Each and every branch was traced from the origin to the termination. Specimens with topographical derangements were excluded from the study. The variations in the branching pattern of the coeliac artery were observed in fourmale cadavers and the rest of the cadavers showed the normal branching pattern.
4. Results
In the present study the trifurcation of the coeliac trunk into usual three branches, the LGA, the CHA, and the SA was observed in all the cadavers except four.
The clinically relevant variations of the coeliac trunk in those four male cadavers were as follows:
5. Discussion
Arterial vascularization of the gastrointestinal system is provided by anterior branches at three different levels of the abdominal aorta (the coeliac trunk and the superior and inferior mesenteric arteries). Differences arising during several developmental stages in the embryonic process lead to a range of variations in these vascular structures. Anatomical variations involving the visceral arteries are common and knowledge of them becomes important in patients undergoing diagnostic angiography for gastrointestinal bleeding or prior procedures such as laparoscopy and laparotomy or any major surgeries of upper abdomen. Therefore the variation concerning the CT should be kept in mind during both surgical and non-surgical evaluations. The anatomical variation of the CT or its branches makes it vulnerable to iatrogenic surgery. It enables to distinguish features which merit further investigations.
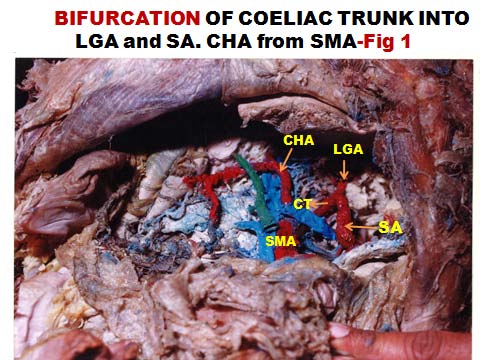
Data derived from past research on cadavers and living persons has shown a plethora of variations. About 15% of the individuals display significant variations form the typical branching pattern of the CT. The CT anatomy in routine examination showed that it can divide into 2-6 branches. Variations in the branches of the CT are most commonly reported once and many authors have reported different variation patterns. Additional branches of the CT other than its normal branches are referred to as collaterals. 3 The pattern of branching of the CT were observed to vary from classical trifurcation, to abnormal trifurcation, bifurcation , quadrifurcation , pentafurcation and even hexafurcation of the trunk.The additional branches of the trunk included the inferior phrenic artery, gastro duodenal artery, middle colic artery, dorsal pancreatic artery, Volume XIV Issue I Version I Year ( ) 2014 I jejunal or duodenal branch.Clinically relevant variations of the coeliac trunk were noted in many cases. 4 Two cadavers showed (Fig- 2 & 4) additional branches i.e. GDA & IPA on right and on left sideThe coeliac trunk is widest ventral branch of the abdominal aorta and its unusual embryological developmentcan lead to very rare about 1%-2.7%, of all anomalies involving the coeliac axis,which arose at the level of L1. 5 The Coeliacomesentric trunkis often fortuitous during autopsy dissections or can be accidently detectedby angiography or abdominal computed topography. The scanning without knowledge of the arterial architecture of the patient in this critical area can lead to surgical risk of error and lethal complications.The injury of the Coeliacomesentric trunk can involve ischemia to both foregut and midgut derivatives. 6 A rare case of absence of the Coeliac trunk.In such casesthe LGA, the SA, the CHA and the SMA arteries arising independently fromthe abdominal aorta. 7 In some cases all the four branches arise from common trunkmeans quadrifurcation of the coeliac trunk.The cadaver in the Fig- 3 The present study showed type 5 (Fig- 1) and type 6 (Fig- 3
6. ) of Adachi & Michel et al classification
The Lipshutz gave a detailed account of the CT based on the mode of origin and distribution of gastric, splenic and the hepatic arteries and classified into 4 types. 9 Type I:(75% cases) The coeliac axis was the common trunk of origin for the LGA, the SA and the CHA.
Type II:(15% cases) The HA and the SA arose from the CT but the LGA had varied origin, either from the HA or directly from the Abdominal aortaType III: (6% cases) The LGA the HA took origin from the CT but the SA was a separate branch from the Abdominal aorta.
Type IV: The coeliac axis was the trunk of origin for the LGA and the SA and the CHA occurred as separate branch from the aorta.
The present study 36 cadavers showed with type I (76%) of Lipshutz classification. This is the normal pattern of branching of CT seen in 31 males and 5 females.
The variations of the CT are common but asymptomatic. They may become important during surgeries and radiological procedures. The CT in addition to LGA, SA and CHA may also sometimes give accessory right hepatic artery and both inferior phrenic arteries. These findings before operation is necessary to avoid post-operative complications and for better accurate radiological interpretations. 10 The bilateral origin of inferior phrenic arteries from the CT was observed in cadaver (Fig- 4) presenting pentafurcation of CT. Similar findings was observed by Petrella et al (34.84%) 10 Knowledge about this variation avoids unintentional sectioning of small caliber arteries during the coeliac artery depression in compression syndrome of the CT by median arcuate ligament.
Classic branching of the coeliac artery into LGA, SA and CHA is seen in approximately 70%. Variations are present in 30% . In general any of the three coeliac branches may arise independently from the Aorta or SMA or coeliac artery may give rise to other branches. 11 Extra coeliac origin of its branches: 12 1) From aorta-LGA 2-3%, SA-<1% and CHA-2%.
2) From SMA-LGA-extremely rare, SA <1% and CHA-2%. VI.
7. Conclusions
The cadaveric findings of the coeliac artery variations and their subtypes in our study is fundamental, that could help to minimize complications related to upper abdominal surgeries This article builds on previous reports and re-emphasizes the importance of coeliac artery variations for useful planning of surgical and radiological procedures of the upper abdomen, including laparoscopic operations of the biliary tract The vascular variations are usually asymptomatic. The background knowledge for the different vascular patterns of the coeliac axis is vital and may become important in patients who undergo coeliacography for gastro-intestinal bleeding, coeliac axis compression syndrome, and prior to operative procedures or transcatheter therapy and for chemoembolization of the pancreas.