1. Introduction
on-Hodgkin's lymphoma is 75% of all lymphomas (1). It is estimated that the incidence in Spain is 10.8 cases per 100.000 women/year, with 2.400 new cases diagnosed per year in women. Ranked seventh in incidence by type of cancer in both men and women, remaining stable in the last years. The likelihood of developing non-Hodgkin lymphoma throughout life is 1 in 51 women.
This disease is found mainly in the lymph nodes or lymphoid tissue and female genital involvement is rare, and can exist in some cases of disseminated disease. The most common gynecologic location is the cervix, followed by uterine corpus and ovaries (2).
Primary cervical lymphoma is a extremely rare entity that presents clinically as cervical cancer, with which we must make a differential diagnosis. Usually presents with vaginal bleeding, dyspareunia and pain. The subtype more frequently described is the large B cells (3).
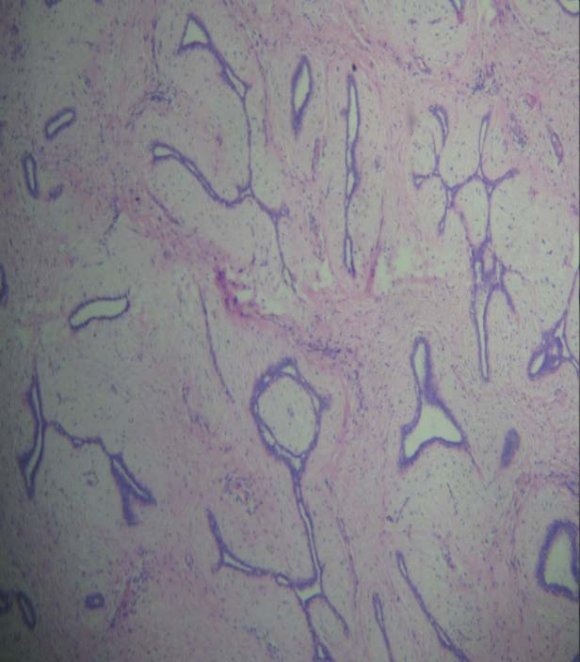
Diagnosis is often difficult because the cytology may be normal, by originate in the stroma with preservation of the scaly surface, obtaining false negatives so taking deep biopsies for histological confirmation is recommended (4).
In early stages the treatment usually more applied is radiotherapy followed by chemotherapy and/or surgery, but in advanced stages and in cases of genital lymphomas chemotherapy seems the best treatment option (5).
We report the case of a patient diagnosed with non-Hodgkin lymphoma of diffuse large B cell uterine location, with good response to chemotherapy.
2. II.
3. Case Report
A 58 year old patient that check in September 2013 per episode of postmenopausal metrorrhagia associated with hypogastric discomfort. As referred only previous bilateral saphenectomy in 2010.
On pelvic examination a bulky tumor that seemed to depend on the posterior lip of cervix showed, this finding was confirmed by ultrasound in which 85mm cervical mass was noted. Given these findings, the following additional tests were requested:
? Pelvic MRI: expansive and infiltrative bulky cervical tumor of 93mm with extension to the uterine body, right parametrium, anterior vaginal wall and dubious infiltration of the rectal wall. Affectation of bilateral pelvic and inguinal lymph nodes rights (Figures 1 and 2). With this diagnosis was prescribed R-CHOP-based chemotherapy regimen receiving 6 cycles from 13/10/14 to 04/02/14. The treatment period was uneventful except for an episode in December 2013 of pneumonia requiring admission for 10 days and was resolved with antibiotic, antiviral therapy, oxygen therapy and noninvasive respiratory support, lagging the 4th cycle of chemotherapy only in 10 days.
At the end of chemotherapy CAT was performed again in March 2014 with almost complete regression of the mass of the uterine cervix, without identifying adnexal masses or supraclavicular, axillary or mediastinal lymph nodes (Figure 6). At present the patient is doing consolidation radiotherapy. Print 6 : Pelvic CAT after the end of chemotherapy regimen III.
4. Discussion
Extranodal lymphomas represent 15% of Non-Hogking lymphomas (6). Of these only 1% originates in the genital tract. So there are no large series to define a standardized treatment. The uterine cervix is the most frequent affected of the genital tract (7), as in our case. Over 75% of cases are diagnosed in premenopausal women, with the average age at diagnosis of 40-44 years (8). Our patient was 58 years old at diagnosis, being well above this age.
To consider as primary lymphoma of the genital tract, the disease should be limited to a single location at the time of diagnosis and there should be no involvement of peripheral blood or bone marrow (9), so after the initial diagnosis obtained with biopsy of the cervical mass conducted a study extension including a bone marrow biopsy and thoraco-abdomino-pelvic TAC, also is advisable to perform a thorough physical examination for suspected peripheral lymphadenopathy. The correct pathologic diagnosis involves making deep biopsies and cytology may have false negatives, as refer Gonzalez et al (10).
The treatment of this condition is controversial because it is a very uncommon condition having few cases reported in the literature. In nodal lymphomas, for patients with localized disease, radiotherapy was the first curative approach and continues to be a part of combined modality therapy (11).
Vaughan et al (12) have shown that almost 70% of patients with localized non-hodking lymphoma can be cured by radioterapy alone. However, the high relapse rate outside the radiation field justifies the requirement of chemotherapy in this setting. A systematic review with meta-analysis the dos Santos et al (13) included four trials with a total of 1.796 patients evaluated chemotherapy alone versus chemotherapy plus radiotherapy and concludes that radiotherapy prolongs progression-free survival, with no impact on overall survival. It must be considered an option for patients who cannot tolerate a high dose or prolonged schedule of chemotherapy.
In advanced stages, the treatment of choice is usually chemotherapy. Neoadjuvant chemotherapy seems an appropriate treatment in cases of genital involvement, according Signorelly et al ( 14 chemotherapy followed by surgery or not, obtained a complete response in 75 % of cases and 5-year survival 90%. Another proposed treatment is the primary chemotherapy followed by consolidation radiotherapy, Marco Bravo et al (15) reported 2 cases of cervical lymphoma treated with CHOP chemotherapy regimen, followed by radiation therapy with complete remission in both cases without evidence of disease 23 and 70 months, respectively. In our patient, after the assessment session with clinical tumor board, this was the chosen treatment.
In the current era in which the target therapy appear promising, there have been encouraging results with rituximab, a monoclonal antibody directed against the CD20 antigen expressed by most of these tumors (16).
We thought that since it is a disease so rare, further investigation is needed in this regard bringing more cases to know what is the best treatment we can offer these patients.
IV.
5. Conclusions
Primary lymphoma of the uterine cervix is extremely rare entity. Usually require the completion of deep biopsies for correct diagnosis at the high rate of false negative cytology. They have rapid growth and most have more than 4cm at diagnosis. It is recommended that thoraco-abdomino-pelvic CAT and bone marrow biopsy to rule out disseminated disease. The standard treatment has not yet been established but more often in advanced stages and genital involvement chemotherapy is the treatment of choice. Genital lymphomas appear to be less aggressive than nodal lymphomas with high overall survival, especially in early stages