1. Cancellation of Elective General Surgical Operations at the Day of Intended Surgery
Ahmed A Elrahman ? , Aamir A Hamza ? & Mohayad A El-Haj ? Abstract-Background: Cancellation of surgical operations in hospitals is a significant problem with many undesirable consequences. Cancelled operations can annoy patients and their families. They are a major drain on health resources, increases theatre costs, results in wasted operating room time and decreases efficiency.In spite of the extensive available literature on preparation of surgical patients and performance of surgical procedures, the focus given to the cancellation of planned surgical operations has been quiet restricted globally.
Objectives: To determine the magnitude and point prevalence of surgery cancellation in patients scheduled for elective operation and it`s different reasons.Patients and methods: A prospective cross sectional study carried out in Omdurman teaching hospital for all patients scheduled for elective general surgical operations in one year (2012 August -2013 August).
Results: During the study 2750 patients were scheduled for general surgical operations, 2460 (89.5%) patients were operated on their planned date. A total of 290 (10.6%) operations were cancelled.Mean age was 41.2 ± 16.5 years with female to male ratio 1.2:1. There were many reasons for postponement of surgery; the main reasonswere categorized into medical related, patient related, administrative, inadequate preparations of patients and other reasons accounted for 30%, 25.5%, 21%, 19.7% and 3.8% respectively. The major three causes for cancellation in the study were; failure of the patients to attend uncontrolled high blood pressure and overloaded schedule, these were seen in 57 (19.7%), 35 (12.1%) and 32 (11.0%) respectively.Most of the reasons 76.9% were potentially avoidable. Conclusion: It was obvious that most of the reasons of postponement of elective general surgical operations were avoidable and can be prevented by simple steps.Cancellations can be minimized if the patients with medical problems were detected early and referred for an anaesthetic assessment soon after they are scheduled for surgery.
2. I. Introduction ost of the surgeries in Omdurman Teaching
Hospital are being performed at a low cost. This means a huge number of patients most of whom belong to lower socio-economic class and travelling from far areas, arriving to be operated.
Elective surgery is an important part of a hospital's workload. Unanticipated postponement on the day of surgery is a tremendous emotional as well as econo-mical trauma for such patients in addition to causing an increase in operation theatre costs and decrease in its efficiency (1) .
Cancellation of surgical operations in hospitals is a significant problem with many undesirable consequences. Cancelled operations can annoy patie -nts and their families. They are a major drain on health resources, increases theatre costs, results in wasted operating room time and decreases efficiency. However, the performance of a surgical operation on schedule requires a complex process of logistics. In spite of the extensive available literature on preparation of surgical patients and performance of surgical procedures, the focus given to the cancellation of planned surgical operations has been quiet restricted globally (2) .Elective surgery is an important part of a hospital's workload. Whenever a case is put on list, it involves interaction of a number of people and in the same way its postponement affects many parties (3) .Different definitions of cancellation exist in the international literature (4) . Some authors define 'cancellation' as only those procedures that were cancelled on the day on which surgery was scheduled, whereas others also include those that were cancelled on the previous day (5,6) .
3. II. Patients and Methods
This is a prospective, cross sectional, descriptive, hospital-based study that was conducted at Omdurman Teaching Hospital over one year (2012 Aug to 2013 Aug). All patients scheduled for different elective general surgical procedures during the time of study were enrolled. Non-probability sampling, with total coverage during the study period was adopted. Included were patients scheduled for elective general surgery after accepting the given informed consent. All patients scheduled for emergency surgery or subspecialty surgical procedures were excluded. Predesigned questionnaire was used for data collection. Variables included patient's characteristics, type of operation, medical related reasons, inadequate preparation of patient, administrative related reasons, patients related reasons and others. The collected data was processed, and analyzed statistically using SPSS computer package version 20.0. Percentages were calculated & Chi-square test was used to analyze the M difference between the various groups. Statistical significance was accepted for P < 0.05. Preoperative consent was obtained from patients together with hospitals approval ethical clearance.
4. III. Results
5. a) Patients' demographics
A total number of 2750 patients were scheduled for general surgical operations; most of them 2460 (89.5%) were operated upon on planned date. A considerable number 290(10.6%) of operations were cancelled. Four operation lists were lost completely due to vacation.
Females were predominant 161(55.5%), with female: male ratio of 1.2:1.The mean age was41.2 ± 16 years and (range2 -80 years). Most of the patients 180 (62.0%) were in the age group 21-50 years (Table 1). Total 290 100
6. b) Categories of cancellation
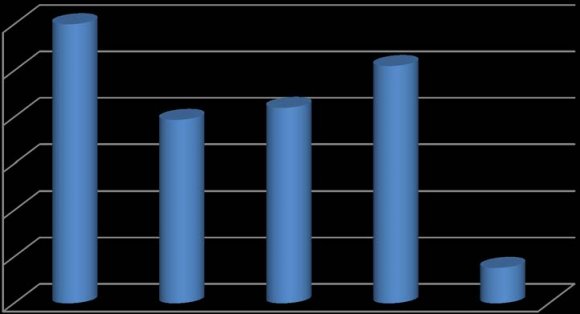
There were many reasons for postponement of surgery and were categorized into medical related, patient related, administrative, inadequate preparations of patients and other reasons. Medical and patients related reasons were the commonest and accounted for 30%, 25.5% respectively (Figure 1). The most common medical related reasons for cancellation were; high blood pressure (39.8%), change of treatment plan (22.7%) and haemoglobin less than ten gram/dl (12.3%) of cancellationswithin this category. Other causes with lesser percentage included; uncontrolled Diabetes Mellitus, upper respiratory tract infection, ischemic heart disease (Table 2). e) Administrative related reasons
The most common administrative reason for cancellation was shortage of time to cover the whole list of operations, which accounted for 11% of all cancellations and more than half the reasons within this category.Failure of equipment needed to conduction the specific operation or no water supply accounted for 13.6% each (Table 2).
7. f) Inadequate patient preparation reasons
Blood not arranged or unavailable in 57.1% and some investigations not done 42.5% were the major contributing factors for surgery cancellation in this group. However drugs not arranged, poor gut preparation for colonic surgery or uncontrolled thyroid patients were the reasons for few elimination (Table 2).
8. g) Other reasons for cancellation
Admission errors or absent consultant surgeons constituted one percent each from the total cancelations (Table 2)
9. IV. Discussion
Surgical cancellation is scheduled surgery which is not done at intended date.An efficient surgical service should have a low rate of cancellation. If operations are cancelled, the Operation Theatres (OT) are underused, efficiency is jeopardized, waiting list increases and cost rises (7) .The National Audit Office in Britain examined five district health authorities in detail and concluded that Operation Theatres were being used half their capacity in spite of huge waiting lists (8) .Most operations are cancelled at 24-hour notice (9) . The patients and the relatives feel disappointed, frustrated, and anxious (10) .
10. a) Cancellation rate
In this study the cancellation rate(CR) of elective general surgical operations was 10.6 % which is similar to a previous report from a developing country (11). However, cancellation rates ranging between 19% and 33% were reported from other developing countries (12, 13), compared to rates between 11% and 24% from developed countries (14,15).The cancellation rate found in this study was compared to cancellation rates reported by different authors (Table 3). Hand R, et al. (14) 1990 USA 17.0% Magbool G, et al. (11) 1993 Saudi Arabia 09.1% Lacqua MJ, Evans JT (23) 1994 USA 17.0% Cavalcante JB (12) 2000 S. America 33.0% Aguirre-Cordova JF (15) 2003 Mexico 24.0% Fersch MB, et al. (24) 2005 USA 13.0% Schofield WN, et al. (25) 2005 Australia 11.9% Paschoal ML, Gatto MA (13) 2006 Brazil 19.9% Sanjay P, et al. (26) 2007 UK 14.0% ZafarA,et al. (27) 2007 Pakistan 25.0% Doumi EA, et al. (1) 2008 Sudan 09.9% current study * 2013 Sudan 10.6%
In the present study, the most common types of cancelled operations were thyroid, breast, hernias and anorectal conditions.For a multi-dimensional problem such as surgical cancellations, it is important to address major reasons that result in cancellations.
11. b) Medical related reasons
Among medical related reasons (MRR) uncontrolled high blood pressure (HBP) is commonest reason accounted for35 (12.1%) cancellation. Hypertension is certainly associated with an increased risk of perioperative morbidity and mortality and a diastolic blood pressure of 110-115 mmHg was considered as a cutoff for postponing anaesthesia (16) .Doumi EA, et al. in El Obied Teaching Hospital in Western Sudan also found that HBP is commonest MRR accounted for 22.2% (1) , as well as reported in similar study in London (17) .
Majority of elective patients were seen by the anaesthetist only on the day prior to surgery. So the preoperative optimization is done over a short period of time. Studies have shown that preoperative anaesthesia assessment of patients inanaesthetic assessment clinics significantly reduces operative room delays and cancellations (18) .
The uncertainty of the highest safe blood pressure for anaesthesia results in variations in practice (19) .
The second reason in MRR is change treatment plan due to recent change in clinical status which account for 6.9 % in our study and showed to be 7.4% in Doumi EA, et al. study (1) . c) Patient related reasons Failure of patient to attend is the commonest cause in this category and accounted for 57 (19.7 %). This could be attributed to fear of operation due to inadequate psychological preparation.A similar significant number found in study done in Nigeria by A.S Oguntol, et al. (19) (20).
12. d) Administrative related reasons
Considering administrative related reasons (ARR), shortage of time accounted for 32 (11%)of the operation cancelled. This found to be gre -ater than 5.6% inWestern Sudan (1) and 1.2% in Nigeria (19) studies and less than that of William, et al. study 18.7% (20) . Lack of anaesthesia staff, power break down and no water supply were the other ARR.When analyzed these reasons were due to failure of the hospital administration to recognize the needs of the operative theatre and the indifferent attitudes among the theatre staff.
A lot of precious time was lost in-patient transport in or out of the operative theaters (OT), in induction of anesthesia, in surgical preparation and draping. The room turn over time may be also reduced if more recovery room beds were made available (21) . In a recent study it was found that only 7%the surgical procedures were started on time (22) .
Training and delegation of responsibilities to young motivated qualified nurses as 'Sister-in-charge' to take over the administrative responsibility of the operating theater might help to overcome the problem. The most common inadequate patient preparation reasons (IPPR) was some investigations not done which accounted for 6.9% of all cancellations.This reflects the reluctance of surgical staff and lack of collaboration with anaesthetic staff.Although this is low compare with 7.1%-27.2% in other different studies (1,19) . Incomplete investigations also could be secondary to lack of funds to pay for the tests rather than inefficiency of the laboratories, though occasionally lack of reagents, poor electricity supply are common causes in the developing countries.
13. Volume XIV Issue III Version I
Blood not arranged is a second common reason in IPPR, accounted for 5.2% which is greater than 0.4% (1) and less than 11.2% (19) .
Phobia for blood donation by patient relatives and the public at large, prevent adequate stocking of our blood banks, thus blood not easily made available for surgical procedures. There is a need to reawaken the usual mass donation by groups of students, civil servants, societies and associations. Auditing of blood usage during surgical procedures should be carried out in various centers in order to really determine what should be the minimum number of units to be requested for procedures.
Lackof surgeons and admission errors, accounted for one percent each, thiswas another reason for cancellations.It is rather higher than 0.6% for absence surgeon and 1.2% for admission error in other study (1) . This occurred in units where team leaders were either part time employees, involved in hospital administration or reporting late due to long distance travels. Adequate staffing of surgical teams and theater workers including porters shall reduce the time wastage thus enhancing efficiency.
Unplanned admissions and lengthy OT lists prepared by junior surgeons, who were not familiar with the procedures, was also a reason for operation cancellation. Many patients did not need surgery or required further work up before surgery. Ensuring that only consultants book patients for surgery would reduce the number of cancellation due to incorrect indication of surgery with significant impact on operating time available. Influence of surgeon experience was observed in this study and found inexperienced surgeons add significantly to the operation time. Consultants were quicker and their presence reduced the likelihood of complications, thus reduced operative time. Moreover it was observed that if a consultant surgeon and consultant anaesthetist were present in OT, the list is likely to proceed with fewer delays (19) .In our study most of surgeries were cancelled at the intended date 53.8% which reflect the importance of preoperative rounds. f) Avoidable causes of cancellation Schofield, et al.2005 classified the causes of cancellation of operations as avoidable and non-avoidable (11) .In our study non avoidable causes were recent clinical changes in the patient's condition, patient who didn't show up, inability to pay fees, cancellation by the patient and cancellation due to emergency priority accounted for 23.1%. Accordingly the majority of our cancellations76.9% were potentially avoidable.
At another study performed at ambulatory surgery practice in the United Kingdom, reasons for can cellation were: acute medical conditions in 23.3% of cases, personal decision of the patient to refuse programming in 22.2%, non-attendance in 2.1%, failure to follow pre-operative guidance in 23.3% and unavailability of resources in 29%. These causes were preventable or possibly preventable in 57.1% of cases, difficult to prevent in 29% and not preventable in 13.9% (6) .
14. V. Conclusion
It was obvious that most of the reasons of postponement general surgical operation were avoidable and can be prevented by simple steps. Cancellations can be minimized if the patients with medical problems were detected early and referred for an anaesthetic assessment soon after they are scheduled for surgery.
In order to enhance cost -effectiveness and efficiency;efforts should be made to prevent unnecessary postponement through careful planning aimed at increasing operation theatre spaces and efficient utilization of few available hospital resources including that of the operating room, theatre facilities and valuable man power improving the scheduling and admission procedure is required for better use of hospital resources.
15. Volume
| Age (years) | Frequency | Percent |
| 2-10 | 7 | 2.4 |
| 11-20 | 26 | 9.0 |
| 21-30 | 60 | 20.7 |
| 31-40 | 59 | 20.3 |
| 41-50 | 61 | 21.0 |
| 51-60 | 36 | 12.4 |
| 61-70 | 34 | 11.7 |
| 71-80 | 7 | 2.4 |
| Medical reasons | Frequency Percent | ||
| Within Total | Within Category | ||
| High Blood pressure | 35 | 12.1% | 39.8% |
| Diabetes mellitus | 07 | 2.4% | 07.9% |
| Upper Respiratory tract infection | 03 | 1.0% | 03.4% |
| Anaemia | 11 | 3.8% | 12.5% |
| Ischemic heart disease | 03 | 1.0% | 03.4% |
| Unfit for medical condition | 04 | 1.4% | 04.5% |
| Change of treatment plan | 20 | 6.9% | 22.7% |
| Abnormal laboratory results | 04 | 1.4% | 04.5% |
| Patient taking aspirin | 01 | 0.3% | 01.1% |
| Total | 88 | 30.3% | 100% |
| Patient related reasons | |||
| Patient failed to attend | 57 | 19.7% | 77.5% |
| Patient refusal | 6 | 2.1% | 08.1% |
| Financial problems | 9 | 3.1% | 12.2% |
| Total | 74 | 24.9% | 100% |
| Administrative related reasons | |||
| Overload schedule | 32 | 11.0% | 54.3% |
| Lack of Anesthetists | 10 | 3.4% | 16.9% |
| Equipment failure | 8 | 2.8% | 13.6% |
| Power breakdown | 1 | 0.3% | 01.7% |
| No water supply | 8 | 2.8% | 13.6% |
| Total | 59 | 20.3% | 100% |
| Inadequate patient preparation | |||
| reasons | |||
| Medicine not arranged | 1 | 0.3% | 02.1% |
| Poor gut preparation | 5 | 1.7% | 10.6% |
| Patient not euthyroid | 3 | 1.0% | 06.4% |
| Anesthesia work-up need | 1 | 0.3% | 02.1% |
| Some investigation not done | 20 | 6.9% | 42.6% |
| Blood not available | 12 | 4.1% | 25.2% |
| Blood not arranged | 15 | 5.2% | 31.9% |
| Total | 47 | 17.5% | 100% |
| Other reasons for cancellation | |||
| Failure of administer anesthesia | 2 | 0.7% | 15.4% |
| Referral to other consultant | 2 | 0.7% | 15.4% |
| Operation not required | 1 | 0.3% | 7.70% |
| Failed intubation | 1 | 0.3% | 7.70% |
| Admissions error | 3 | 1.0% | 23.0% |
| Operated elsewhere | 1 | 0.3% | 7.70% |
| Others | 1 | 0.3% | 7.70% |
| Lack of staff of surgeons | 3 | 1.0% | 23.0% |
| Total | 13 | 4.6% | 100% |
| Author | Year | Country | Cancellation rate |