1. Introduction
he human heart is an exceptional organ, that's designed to function continuously for an average 70 year life span of a normal individual, thus a human heart beating at a rate of 70 beats per minute will exceed 2.5 billion beats throughout the life span of a human being (McCartan et al., 2012), this exceptional muscular pump displays extraordinary capacity to adapt to a broad range of genetic and extrinsic factors to sustain its contractile functions, failure to do so results in cardiac dysfunction and cardiomyopathy (Harvey and Leinwand, 2011). Cardiomyopathies are defined as "a heterogeneous group of diseases involving the myocardium which are associated with mechanical and/or electrical dysfunction that usually exhibits inappropriate ventricular hypertrophy or dilation and are due to a variety of causes that frequently are genetic" Author ?: Hawler Medical University. e-mail: [email protected] (Maron et al., 2006). They can be classified either into primary, or secondary; or according to the type of cardiomyopathy into dilated cardiomyopathy (DCM), hypertrophic cardiomyopathy (HCM), restrictive cardiomyopathy (RCM), and arrhythmogenic right ventricular cardiomyopathy (ARVC) (Wexler et al., 2009) DCM is a progressive, irreversible condition with an estimated prevalence of 1:2500, and is considered one of the leading causes of heart failure (Burke, 2011). HCM is regarded as a leading cause of death among athletes, and has an incidence of 1:500 (Maron, et al., 2006), while RCM and ARVC are considered rare types of cardiomyopathy (Wexler et al., 2009). Many biomarkers have been associated with cardiac remodeling and cardiomyopathy (Gopal and Sam, 2013), among these is the cTn-I and MMP-9, their elevation is involved in cardiac injury and cardiomyopathy (Herman et al., 1999;Fairweather et al., 2011), in addition the renin angiotensin system (RAS) can induce left ventricular hypertrophy and fibrosis (Ocaranza et al., 2002), due to the direct effect of Ang II on myocardial cell hypertrophy through its action on the AT 1 receptor (Mehta and Griendling, 2007).
2. II.
3. Materials and Methods
Thirty six female albino rats, 8-12 weeks old, weighing 140-200 grams, were used. The animals were housed in groups of four per cage, on sawdust in the animal house facility, under conditions of controlled ambient temperature of 22-25 oC with a 12 hour light/ dark cycles. The animals were supplied with rodent chow and free access to tap water.
a) The Rats were allocated into 3 groups as follow Group 1: (Control group) This group included 8 rats and served as the control group; they received 1ml distilled water orally via oral gavage and 0.5 ml distilled water subcutaneously for a period of 14 days. Group 2: (ISO group) included 8 rats and served as a model of isoproterenol induced cardiomyopathy. The animals were injected with isoproterenol hydrochloride in a dose of 5mg/kg/day (Tipnis et al., 2000;Heather et al., 2009;Chowdhury et al., 2013), S.C. for a period of 14 days to induce distinguishable cardiac hypertrophy and cardiomyopathy. Group 3: (Treatment group) included 20 rats, and served as the treatment group; they were T b) Serum Measurements Rat Matrix Metalloproteinase 9 and Cardiac troponin I serum concentrations were measured bydouble-antibody sandwich enzyme-linked immuneosorbent assay (ELISA), purchased from Uscn life science/ Germany and QAYEE-BIO/ Germany respectively.The Hw/Bw ratio was calculated by dividing the heart weight (mg) over the body weight (gm.). (Suckowet al, 2005).
????\???? ð??"ð??"ð??"ð??"ð??"ð??"ð??"ð??"ð??"ð??" = ?????????? ???????????? ???? ???? ??ð??"ð??"???? ????ð??"ð??"????ð??"ð??" ð??"ð??"?? ???? c) Statistical AnalysisAll data are expressed as Mean ± standard deviation. Data was analyzed using the Statistical Package for Social Sciences (SPSS) version 16. Data analysis was made using one-way analysis of variance (ANOVA). Comparison between groups was done by using Post Hoc LSD test. P?0.05 was considered statistically significant.
4. III.
5. Results
By the end of the study the following mortality was recorded: 2 of 10 rats in the ISO-Cand group. These animals were excluded from the study.
The table below shows the effect of coadministration of the treatment drugs with isoproterenol on the studied parameters. Irbesartan in its respective group, significantly reduced mean serum MMP-9 concentration to 8.10±2.32 ng/ml, while candesartan significantly reduced both serum concentrations of MMP-9 (8.25±1.96 ng/ml) andcTn-I (67.47±10.06 ng/ml,). The Hw/Bw ratio was significantly reduced by both treatment drugs. The Cardioprotective Effects of Irbesartan and Candesartan in Isoproterenol Induced Cardiomyopathy in Rats further subdivided into 2 subgroups all of which received isoproterenol as stated previously for group 2, along with the treatment drug administered via oral gavage, and they include: Group 3.1 (ISO-Irb. group): This group included 10 rats that were given irbesartan 50mg/kg/day. Group 3.2(ISO-Cand. group): This group included 10 rats that were given candesartan 2.6 mg/kg/day. All groups were treated for a period of 14 consecutive days. Isoproterenol hydrochloride solution was prepared by reconstitution of isoproterenol hydrochloride powder with distilled water daily under sterile conditions immediately before injection (Grimm et al., 1998). The rats were first weighed and then isoproterenol was injected S.C into each rat except control group which was injected with distilled water S.C. The subcutaneous route was used because of the higher levels of cTn-I associated with this route, and a greater degree of cardiac injury (Brady et al., 2010). Immediately after the injection, the rats received the corresponding treatment drug according to the stated dose for each group, (except for the control group and the ISO group). After 14 days, 24hr of the last dose, the rats were anesthetized by injecting thiopental sodium 100mg/kg/I.P (Grimm et al., 1998), then dissected to expose the beating heart, after which blood was withdrawn directly from the right ventricle. The withdrawn blood was placed in a graduated glass conical bottom centrifuge tubes and allowed to settle for 20 min after which it was centrifuged at 3000 RPM for 10 minutes. The obtained serum was placed in eppendorf tubes and stored at -20 oC for further analysis; the heart was extracted, dried with filter paper and weighed.
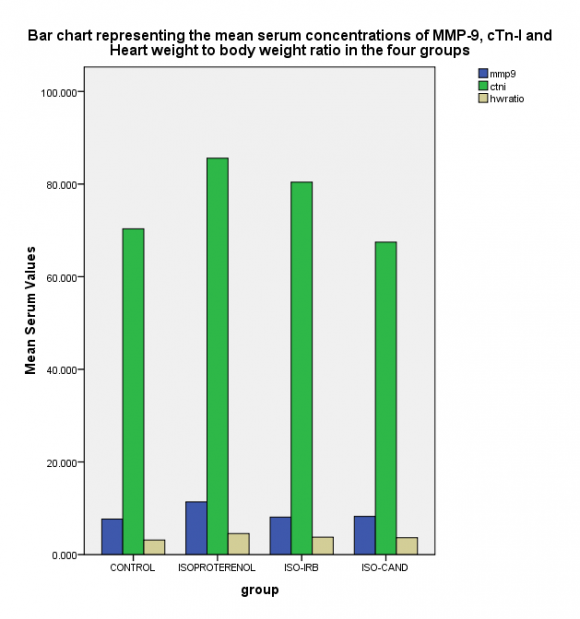
| MMP-9 ng/ml | cTn-I ng/ml | Hw/Bw ratio | ||
| Groups | Control ISO ISO-Irb | 7.66±1.50 11.38±3.41 * 8.10±2.32 a | 70.35±13.27 85.58±10.95 * 80.42±14.07 | 3.15±0.35 4.53±0.31 * 3.76±0.29 a |
| ISO-Cand | 8.25±1.96 a | 67.47±10.06 ab | 3.65±0.20 a | |
| P-Value | 0.015 | 0.019 | <0.001 |