1. Introduction
pontaneous retroperitoneal hemorrhage is an uncommon entity. It is even rarer when the underlying cause is associated with renal disease (1). Sp ontaneous rupture of the kidney affects either the collecting system or parenchyma and, in most cases, the non-traumatic rupture is associated with underlying diseases of the kidney (2). We rep ort a case of spontaneous rupture of left kidney with massive retroperitoneal hematoma secondary to multiple simple renal cysts presented with hemorrhagic shock in a patient on anticoagulation therapy.
2. II.
3. Case Report
An 85-year-old man was presented to our emergency department because of left flank pain and an increasing mass in his left flank of one day duration. He i s known hypertensive and diabetic on medical treatment. His urological history was normal and he did not have a hist ory of trauma. Two months earlier to his presentation he had confirmed deep vein thrombosi s of the left femoral and popliteal veins and he was put on enoxaparin 60 mg subcutaneously twice daily. On examination he was c onscious but drowsy. Pulse was 110/minute; blood pressure was 100/40 mm of Hg. Abdominal examination showed a palpable mass and tenderness over the left flank. There was no hematuria on urine analysis. Hemoglobin was 8.4 gram%, WBCC 20x10 9, urea 18.6mmol/L and creatinine 289 mmol/L. coagulation studies were normal.
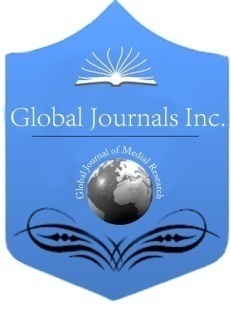
After initial fluid resuscitation he had a noncontrasted CT scan which showed Left perinephric and retro peritoneal slightly dense (about 60 HU) fluid collection which measure about 19 x 4 cm extending down to the left upper pelvic region, together with a hypodense cyst( measures about 6 x 6.7 cm) in the upper pole of the right kidney. The left psoas muscle is slightly larger in size than the right one and it is bordering the left retroperitoneal fluid collection (figure 1-2). The patient was admitted to the ICU and continued to be resuscitated with blood and fresh frozen plasma. Inspite of 3 units of blood transfusion he dropped his hemoglobin to 5.4 gram% together with obvious increase in the left flank mass size. A decision was taken to go ahead with CT angiography with a possibility of percutaneous embolization of the renal artery. The CT angiogram showed a significant increase in the amount of the left renal, perirenal and retroperitoneal hematoma with evidence of contrast extravasations from renal cortex at different sites in the arterial and provenous phases denoting active bleeding associated with poor left renal excretion. The retroperitoneal hematoma is extending caudally to the left lower pelvis along the anterior aspect of the left psoas muscle together with mild free intraperitoneal fluid. Multiple small renal simple parenchymal cysts and double left renal arteries were noted. There was 7 x 6 cm right renal simple cyst (figure 3-5). In view of c ontinuous dropping of the hemoglobin, expansion of the retroperitoneal hematoma and the CT evidence of active bleeding the patient were taken for emergency exploration through transperitoneal approach. Intra operatively there was extensive retroperitoneal hematoma extending from sub splenic region down to the pelvis and a huge cortical rupture on the posteriolateral aspect of the left kidney together with multiple ruptured and intact renal cysts (photo 1-3). The left ureter was of normal caliber and there was no evidence of backward s pressure on the renal pelvis. Left nephrectoy was done together with evacuation of the retroperitoneal hematoma and drainage of the retroperitoneal space. Postoperatively the patient had percutaneous insertion of inferi or vena cava filters to prevent pulmonary embolism and was commenced on heparin subcutaneously. He remained haemodynamically stable and he didn't require further blood transfusion. The histopathol ogy of the kidney revealed focal glommerulosclerosis with focal interstitial inflammation and ruptured multiple simple cortical cyst s. There was no evidence of malignancy.
4. Global Journal of
5. Discussion
Definition of Wunderlich syndrome, also known as sp ontaneous retroperitoneal hemorrhage, was first given in 1700 by Bonet and was more completely explained by Wunderlich in 1856 (3). Etiologies as well as the preci se mechanisms leading to Sp ontaneous nontraumatic massive retroperitoneal hemorrhage are unclear in most of the reported cases (4). It i s usually secondary to a renal neoplasm, with angiomyolipoma being the most frequent followed by renal cell carcinoma (5) occurring in 57-73% of cases (6).
It also seen in association with patients with anticoagulation therapy, bleeding abnormalities, and hemodialysis (7) and may represent one of the most serious and potentially lethal complications of anticoagulation therapy. The incidence of retroperitoneal hematoma has been reported at 0.6-6.6% of patients undergoing therapeutic anticoagulation (8, 9, and 10). Warfarin, unfractionated and l ow-molecular weight heparin have all been implicated (11).
Non-traumatic retroperitoneal hemorrhage due to a spontaneous kidney rupture is a known, but uncommon, entity (1). Dougal et al examined 78 individual cases of renal rupture. He reported that renal tumor rupture was the cause in 58% of cases, vessel diseases in18% and infections in 10% of all cases of retroperitoneal bleeding (2).
In renal tumors the incidence is high in angiomyolipoma, occurring in 13-100% of the cases, depending on tumor size, while in renal cell carcinoma, it occurs in only 0.3-1.4% of cases (12).
Simple renal cysts are frequent, particularly in the elderly. Fifty per cent of individuals over 50 years of age have single or multiple cysts (13). Simple cysts are discrete lesions within the kidney that are typically cortical, extending outside the parenchyma and distorting the renal contour (14). They can be unilateral or bilateral, single or multiple. They are usually asymptoms. Their complications include ob struction, infection, rupture or hemorrhage, confined either to the cyst or causing subcapsular or peri-renal hemorrhage (1).
Many cases of kidney ruptures were reported in the literature in association with polycystic kidney disease (15)(16), however although renal cysts are commonly seen, sp ontaneous hemorrhage into a cyst causing a massive retroperitoneal hematoma and circulatory compromise i s an extremely rare event (17).
The cause of cyst rupture with hemorrhage is unclear, as it is not known whether expansion with increased intracystic pressure occurs, with the subsequent tearing of blood vessels, or whether hemorrhage into the cyst is the first event, with subsequent rupture from cyst expansi on (1,18).
Although we don't know the exact mechanism of the kidney rupture in our case but we assume that rapid and sp ontaneous bleeding occurred into the cysts, followed by the cysts rupture, and eventually by retroperitoneal bleeding. We al so believe that the prolong use of the enoxaparin contributed significantly to both triggering of the bleeding and the extent of the retroperitoneal hematoma.
Spontaneous rupture of the kidney usually present with classical 'Lenk's triad', consisting of acute flank pain, tenderness and symptoms of internal bleeding (19).
CT angiography i s the gold standard investigation in patient suspected to have sp ontaneous kidney rupture. In addition to confirming the rupture it provides very crucial information that whether the bleeding is continuing or stopped.
Nephrectomy is the treatment of choice in patients with kidney rupture with severe perirenal hematoma and severe retroperitoneal bleeding (20,2). The midline transabdominal approach is preferable as it allows safer vascular c ontrol before exploring the ruptured kidney, and should be considered in patients with signs of a large blood loss from heavy retroperitoneal bleeding. Some authors advocate nephrectomy even if the renal angiogram failed to demonstrate the cause of the hemorrhage due to the possibility of a small clinically unapparent renal cell carcinoma (21, 22, and 23). In contrast, some others have advi sed a conservative approach when diagnostic studies fail to demonstrate a significant pathology (24). Renal arteriography with embolization is anther therapeutic option to control the bleeding in haemodynamically stable patients when renal tumors can be excluded (25).
IV.
6. Summary
Non-traumatic retroperitoneal hemorrhage due to a spontaneous kidney rupture is a known, but uncommon. It i s even rarer when the underlying cause is associated with renal di sease. Sp ontaneous nontraumatic massive retroperitoneal hemorrhage (Wünderlich's syndrome) i s usually secondary to a renal neoplasm, with angiomyolipoma being the most frequent followed by renal cell carcinoma. It is al so seen in association with patients with anticoagulation therapy, bleeding abnormalities, and hemodialysis. Sp ontaneous rupture of the kidney usually present with classical 'Lenk's triad', consisting of acute flank pain, tenderness and symptoms of internal bleeding. CT scan almost always confirms the diagnosis and point out to the cause. Nephrectomy is the treatment of choice in patients with kidney rupture with severe perirenal hematoma and severe retroperitoneal bleeding.