1. Review Article
neumothorax represents a common clinical problem. 1 The development of a pneumothorax with ensuing hypoxia and hypercapnia can be potentially life-threatening event. 2 Correct interpretations of chest radiographs in the clinical setting can be lifesaving! On x ray chest pneumothorax is seen as hyperlucency without lung markings (pulmonary vasculature) and the positive presence of the visceral pleural margin of the partially collapsed lung. A visceral pleural line is seen without distal lung markings. Lateral or decubitus views are recommended for equivocal cases. 3 All that glitters is not gold -similarly all situations with hyperlucency are however not pneumothorax. There are many other causes for hyperlucency on a chest x ray and differentiating them from pneumothorax is crucial. A stepwise approach in reading a chest x ray with hyperlucency will avoid wrong diagnosis and facilitate correct and timely treatment.
Hence it is important for the clinicians to be able to navigate through various causes of hyperlucency. The following flow chart is made specially to help this.
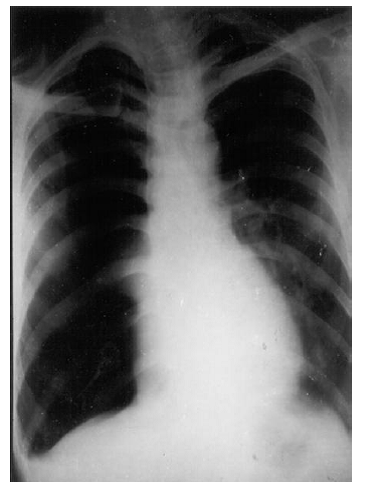
In any x ray start by looking for hyperlucency, absence of lung markings, visceral pleural margin and any fluid level. For example look for figure 1 and analyze the following: Once pneumothorax is recognized, a careful look at x ray may reveal a lot of information about the cause, associated conditions and unravel about underlying lung. 4 However, when we recognizes the presence of pneumothorax we must have a streamlined approach for that. An approach is suggested below. 'Drill' for seeing an X-ray with pneumothorax:
A. Things to look for on the same side of pneumothorax.
B. Things to look for on the opposite side of pneumothorax.
C. Things to look for on both sides.
D. Things to look for under a pneumothorax. ? Surgical emphysema -air in subcutaneous tissues, seen bilaterally, probably as a result of a chest tube (intercostal tube) introduction. Look for a rib fracture whenever there is surgical emphysema.
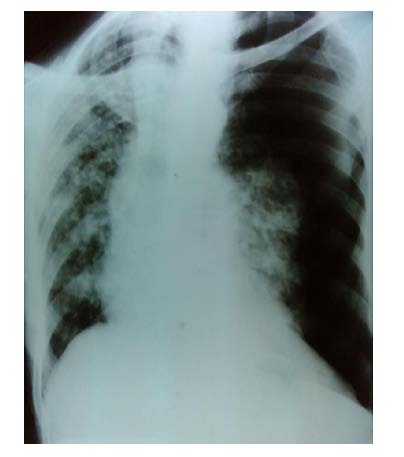
Clinical clue: crepitus in the muscle planes overlying the surgical emphysema. The most obvious finding in this Chest X ray in figure 4 cavity outside the pleura. The hyperlucency is situated lateral to the margin of the collapsed lung (outlined by the visceral pleura). Therefore this hyperlucency is clearly due to presence of free air in the pleural cavity. The simultaneous presence of air and fluid indicated by a horizontal fluid level, helps to identify this situation as a hydropneumothorax. Note that the visible portion of the partially collapsed lung is not healthy-there is an apical cavity. The opposite lung also shows evidence of infiltration. The overall picture strongly suggests possibility of underlying tuberculosis as evidenced by the cavity, whose rupture is most likely the cause of pneumothorax.
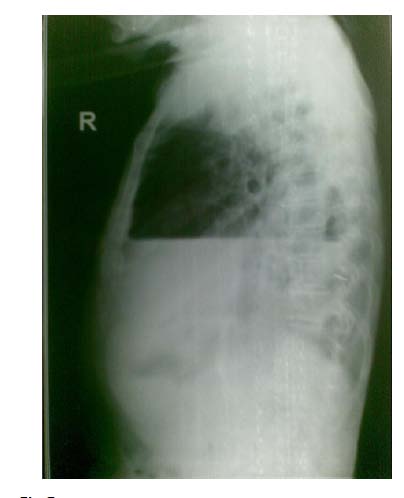
2. Figure 5
There is a clearly seen horizontal fluid level in the lateral view in Figure 5. Above the fluid level there is an area of hyperlucency without lung markings (free air). Margin of the collapsed lung though faintly visible is not seen as clearly as in the PA view.
3. is an example of tension pneumothorax.
There is a lot of free air outside the lung which has collapsed like a deflated balloon to thehilum of the lung(which also shows evidence of some underlying disease). The free air has resulted in hyperlucency without lung markings obviously because the vessels (which would have resulted in visible lung markings) have collapsed to the hilum with the lung. There is lot of free air outside the lung exerting pressure on neighborhood structures resulting in flattening of diaphragm, shift of mediastinum to the opposite side.
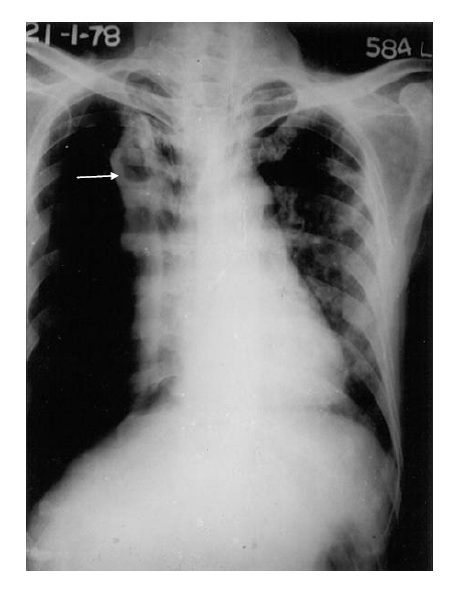
The pressure can also be exerted on the great vessels for which the veins (superior and inferior vena cavae) are more vulnerable (than aorta). This can explain the hypotension and shock which can complicate the tension pneumothorax. Figure 8 In Figure 8 observe: 1. Hyperlucency (unilateral on right side +no lung markings + 2. Margin of the partially collapsed lung. 3. Cavities inside the partially collapsed lung. 4. Tracheal shift to the opposite side. 5. Infiltration in the opposite lung. 6. Cardiac shift to the opposite side.
4. Note of caution:
The scapular margin seen on the left side can erroneously be considered to be margin of the collapsed lung.
5. c) Things to Look for on Both Sides
1. Bilateral pneumothorax: TB, connective tissue disorders. like Marfan's syndrome 2. Look for mediastinal emphysema, surgical emphysema.
Observe in figure 9 Observe in figure 10 ,the smooth outlining of the heart with a radiolucent shadow. This is suggestive of mediastinal emphysema .Also observe infiltration in both lungs.
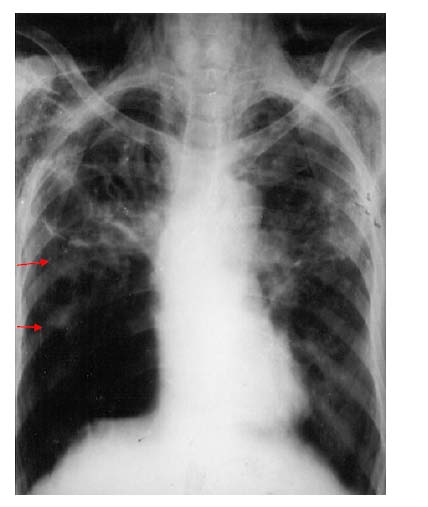
d) Things to Look for "Under" the Pneumothorax 1. Visible lesions can be Infiltration, cavity, in a partially collapsed lung, emphysema(sometimes seen after expansion), bulla etc. 2. "Invisible" lesions: Bulla, sub pleural lesions. Observe in figure 11 ,COPD changes in this long term male smoker of 60 years age.
Notice the pneumothorax at the right lower zone. Though it is a small pneumothorax it is clearly visible -Hyperlucency without lung markings laterally and margin of the collapsed lung covered by the visceral pleura medially. Note the blunted costophrenic angle. What caused this pneumothorax?
Look at the lower zone on the other side (red arrow) -you will observe a hyperlucent circular area but no pneumothorax-a Bulla, which can sometimes mimic a cavity or a pneumothorax. A similar bulla on the right side must have resulted in the Pneumothorax.
Beware of the effects that could have happened but have not:Large pneumothorax + trachea/ Look for a lesion causing heart not shifted to opposite side volume loss in the disorder shifted to the same side eased lung: eg: fibrosis, tumour (an ominous sign when it is due to a tumour).
6. II.
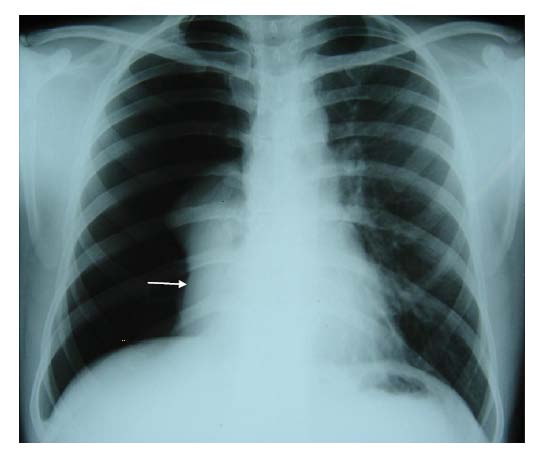
7. Localised Pneumothorax
Please note that in this x ray (figure 12 ) the outline of the collapsed lung margin on the right side is very faint.
This is an example of localized apical pneumothorax. A prominent cardiomegaly and a prominent medial border of the scapula on the left side is two distracting features in this x ray.
In figure 13 we can see close up view of the localized apical pneumothorax. Please observe that free air in the pleural cavity (pneumothorax) is situated between the two (visceral and parietal) layers of pleura. The visceral layer outlines the outer border of the collapsed lung.
The treatment of the pneumothorax and its cause has to be individualized for each patient and is out of scope of this article. However underlying etiology, associated conditions and other information revealed by a X ray can be essential guiding tool in deciding the treatment.
8. III.
9. Conclusion
A close look at x-ray can be highly informative and revealing. To diagnose pneumothorax timely can be life saving. This approach is an attempt to help students and physicians to systematically approach pneumothorax.